Agnew-Blais Jessica, Seidman Larry J
Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA.
Cogn Neuropsychiatry. 2013;18(1-2):44-82. doi: 10.1080/13546805.2012.676309. Epub 2012 Sep 21.
Neurocognitive dysfunction is a central feature of schizophrenia and is observed during all phases of the illness. Because schizophrenia is known to run in families, studying neurocognitive function in first-degree, nonpsychotic relatives has been a widely utilised strategy for almost 50 years for understanding presumed "genetic risk". Studying nonpsychotic relatives ("familial high-risk", or FHR) allows for identification of cognitive vulnerability markers independent of confounds associated with psychosis.
Prior meta-analyses have elucidated the level and pattern of cognitive deficits in the premorbid, prodromal, and postonset periods of psychosis, and in relatives regardless of age. However, no prior quantitative analyses have specifically focused on studies of young first-degree relatives of individuals with schizophrenia who have not passed through the peak age illness risk (<age 30). The English language literature of neuropsychological studies of first-degree relatives for schizophrenia was identified up to 15 May 2011.
From 33 studies, 28 studies met our criteria for quantitative review, utilising >70 individual tests and 250 variables.
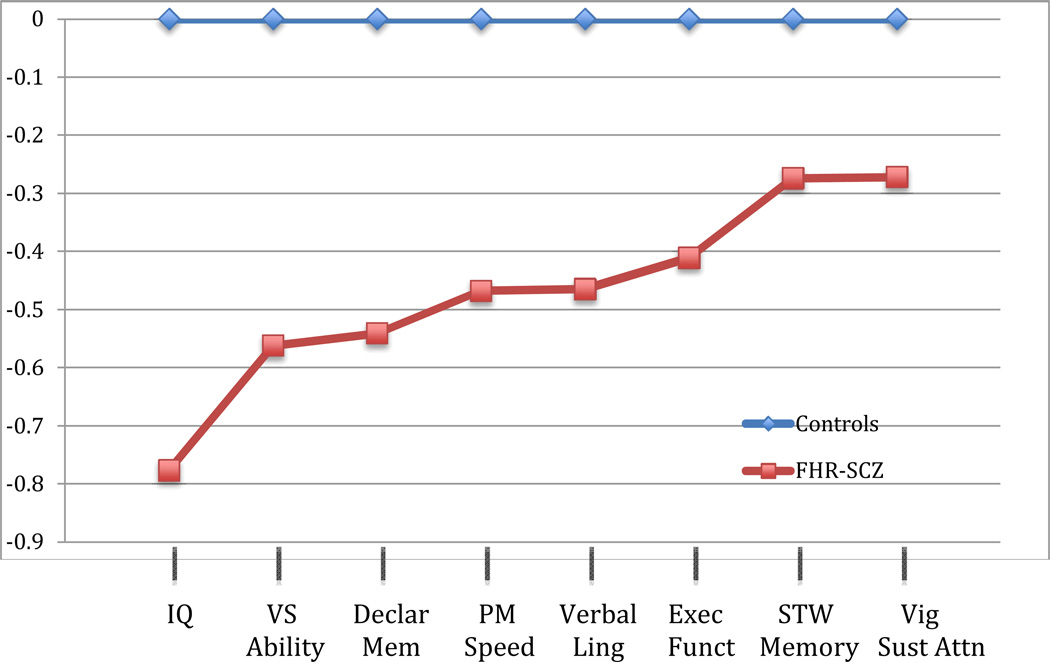
In general, young FHR individuals demonstrated deficits with a moderate level of severity compared with healthy controls. The largest average effect sizes (ESs), based on tests given in at least three independent studies, were on estimates of Full Scale IQ (d= -0.777), followed by Vocabulary (d= -0.749) and single word reading tests (d= -0.698) (often used as estimates of IQ). Measures of declarative memory, sustained attention, working memory and others had more modest ESs. Deficits were milder than in established schizophrenia, but often as severe as in clinical high-risk or putatively prodromal participants and in older relatives examined in prior meta-analyses. Additionally, while assessed from a more limited literature, youth at FHR for schizophrenia tended to show worse neurocognitive functioning than those at FHR for affective psychosis. This suggests that genetic risk for schizophrenia as reflected in a positive FHR carries an especially heavy impact on cognitive ability.
神经认知功能障碍是精神分裂症的核心特征,在疾病的各个阶段均可观察到。由于已知精神分裂症具有家族聚集性,近50年来,研究一级非精神病性亲属的神经认知功能一直是理解假定“遗传风险”的广泛采用的策略。研究非精神病性亲属(“家族高危”,或FHR)有助于识别独立于与精神病相关混杂因素的认知易感性标志物。
先前的荟萃分析已经阐明了精神病发病前、前驱期和发病后以及亲属(无论年龄)的认知缺陷水平和模式。然而,以前没有定量分析专门关注未度过疾病风险高峰期(<30岁)的精神分裂症患者的年轻一级亲属的研究。截至2011年5月15日,已确定了关于精神分裂症一级亲属神经心理学研究的英文文献。
从33项研究中,28项研究符合我们的定量综述标准,使用了超过70项个体测试和250个变量。
总体而言,与健康对照相比,年轻的FHR个体表现出中度严重程度的缺陷。基于至少三项独立研究中进行的测试,最大的平均效应量(ESs)出现在全量表智商估计值上(d = -0.777),其次是词汇(d = -0.749)和单字阅读测试(d = -0.698)(常被用作智商估计值)。陈述性记忆、持续注意力、工作记忆等测量的效应量较小。缺陷比已确诊的精神分裂症患者轻,但通常与临床高危或假定前驱参与者以及先前荟萃分析中检查的老年亲属一样严重。此外,虽然从更有限的文献中进行评估,但精神分裂症FHR的年轻人往往比情感性精神病FHR的年轻人表现出更差的神经认知功能。这表明FHR阳性所反映的精神分裂症遗传风险对认知能力有特别严重的影响。