Division of Sports Medicine, Department of Orthopaedic Surgery, Rush University Medical Center, Rush Medical College of Rush University, Chicago, Illinois.
Sports Health. 2011 Sep;3(5):435-40. doi: 10.1177/1941738111414126.
Osseous injury to the glenoid is increasingly being recognized as one of the most important aspects in the successful management of recurrent shoulder instability. Proper early recognition of glenoid bone injury in the setting of recurrent instability will lead to successful nonoperative and operative decision making, particularly in the athletic patient.
We conducted a MEDLINE search on shoulder instability from 2000 to 2010. The emphasis was placed on patient-oriented Level 1 literature from 2000 to 2010.
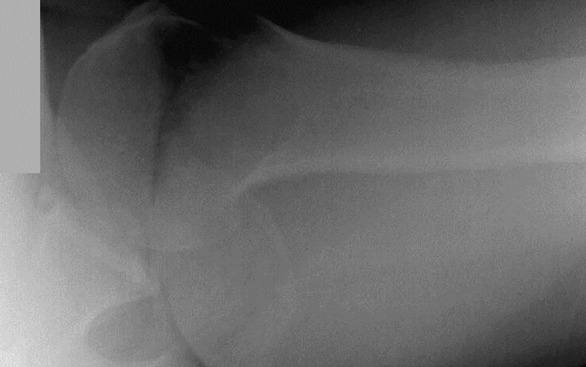
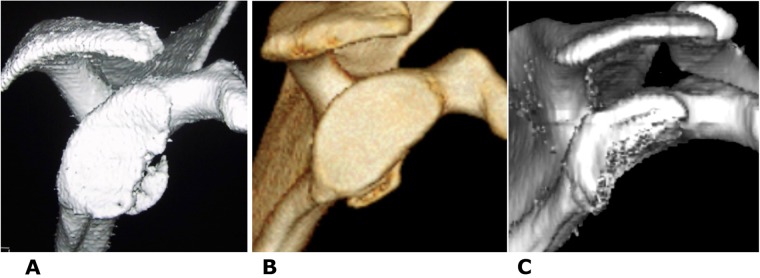
After a traumatic anterior dislocation of the shoulder, the most common structural injury is an avulsion of the anteroinferior capsulolabrum, which is also known as a Bankart lesion. If this specific injury is accompanied by an associated fracture in the glenoid rim, the term bony Bankart lesion is more applicable. With diminished articular constraints, the glenohumeral joint is subject to recurrent instability, thereby potentiating the bony injury cycle. Additionally, patients with osseous defects usually complain of instability within the midranges of motion, or they recall a progression of instability. If glenoid bone loss is present, the humeral head often easily subluxates over the glenoid in the midranges of abduction (30°-90°) and lower levels of external rotation. Imaging workup should begin with plain radiographs, but advanced imaging should be obtained if there is any suspicion of bone loss. Treatment includes both nonoperative and operative interventions.
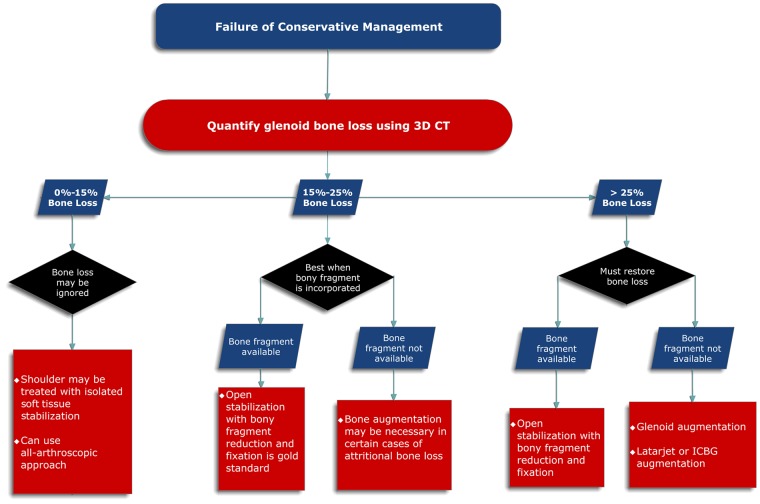
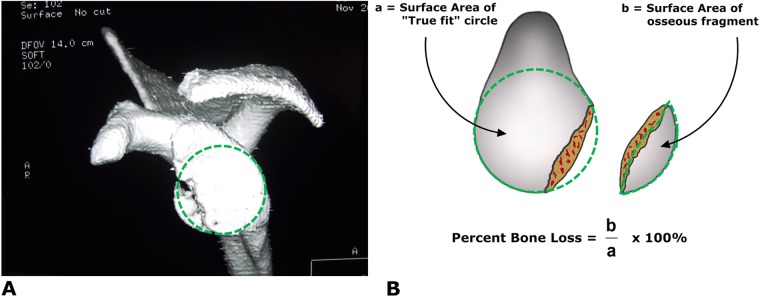
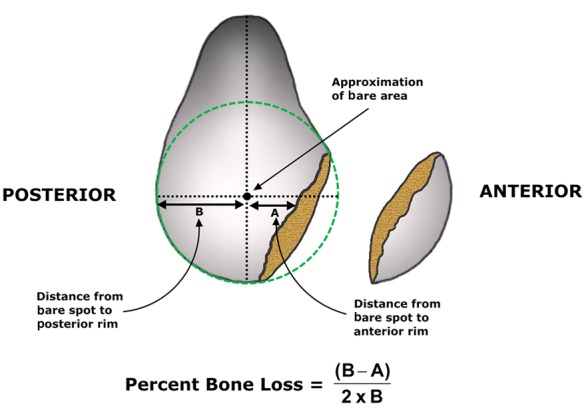
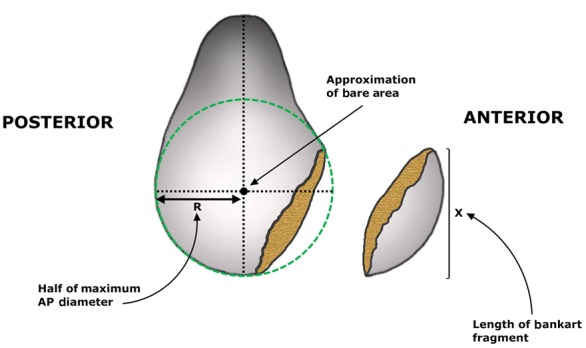
Estimation of the amount of glenoid bone loss and the failure of nonoperative care is essential for guiding management, patient expectations, and surgical decision making.
肩盂骨损伤在复发性肩关节不稳定的成功治疗中越来越被视为最重要的方面之一。在复发性不稳定的情况下,对肩盂骨损伤的早期正确识别将导致非手术和手术决策的成功,特别是在运动患者中。
我们对 2000 年至 2010 年的肩不稳定进行了 MEDLINE 搜索。重点是 2000 年至 2010 年面向患者的一级文献。
在肩部创伤性前脱位后,最常见的结构损伤是前下关节囊盂唇的撕脱,也称为 Bankart 病变。如果这种特定损伤伴有盂唇骨边缘的相关骨折,则更适用骨性 Bankart 病变这一术语。由于关节约束减弱,盂肱关节易发生复发性不稳定,从而增强了骨损伤循环。此外,有骨缺损的患者通常会在运动中段抱怨不稳定,或者他们会回忆起不稳定的进展。如果存在盂骨缺失,肱骨头在外展中段(30°-90°)和较低的外旋水平下很容易向盂唇骨上方半脱位。影像学检查应从普通 X 线片开始,但如果怀疑有骨丢失,应进行高级影像学检查。治疗包括非手术和手术干预。
估计盂骨缺失的程度和非手术治疗的失败对于指导管理、患者期望和手术决策至关重要。