Houston, Texas From the Departments of Plastic Surgery and Diagnostic Imaging, University of Texas M. D. Anderson Cancer Center.
Plast Reconstr Surg. 2012 Oct;130(4):541e-549e. doi: 10.1097/PRS.0b013e318262f115.
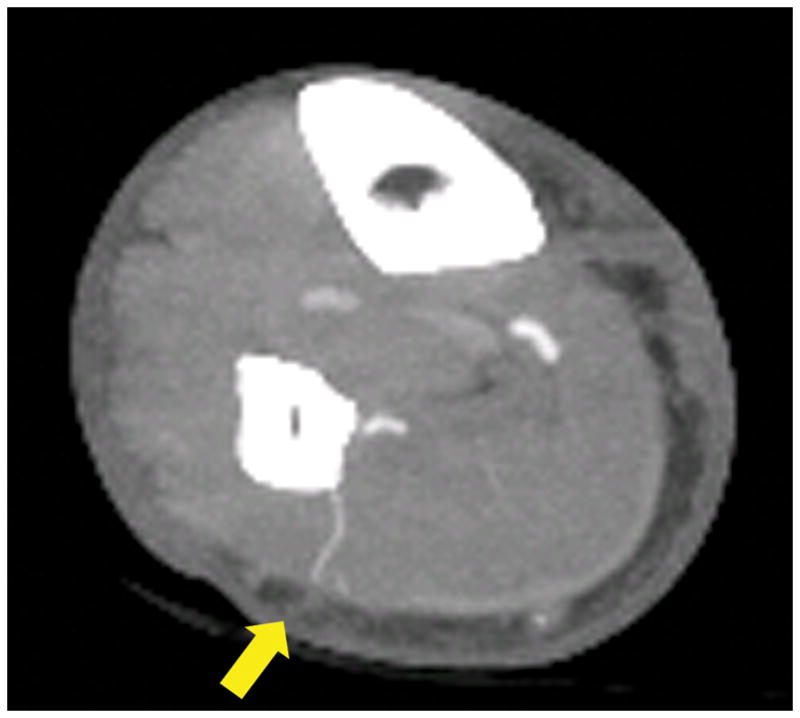
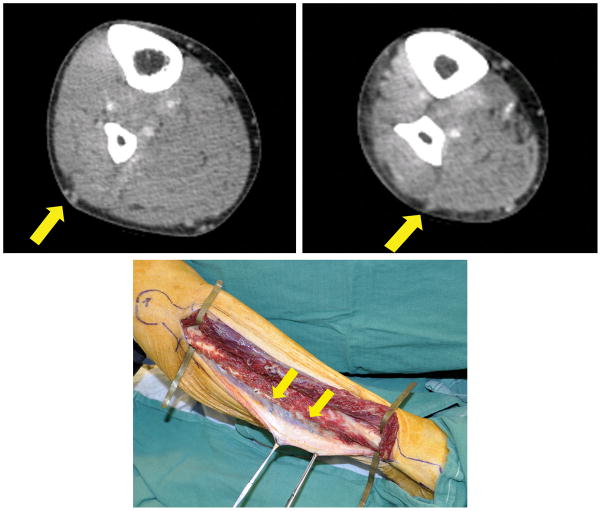
In designing an osteocutaneous fibula flap, poor planning, aberrant anatomy, or inadequate perforators may necessitate modification of the flap design, exploration of the contralateral leg, or additional flap harvest. The authors studied the predictive power of computed tomographic angiography in osteocutaneous fibula flap planning and execution.
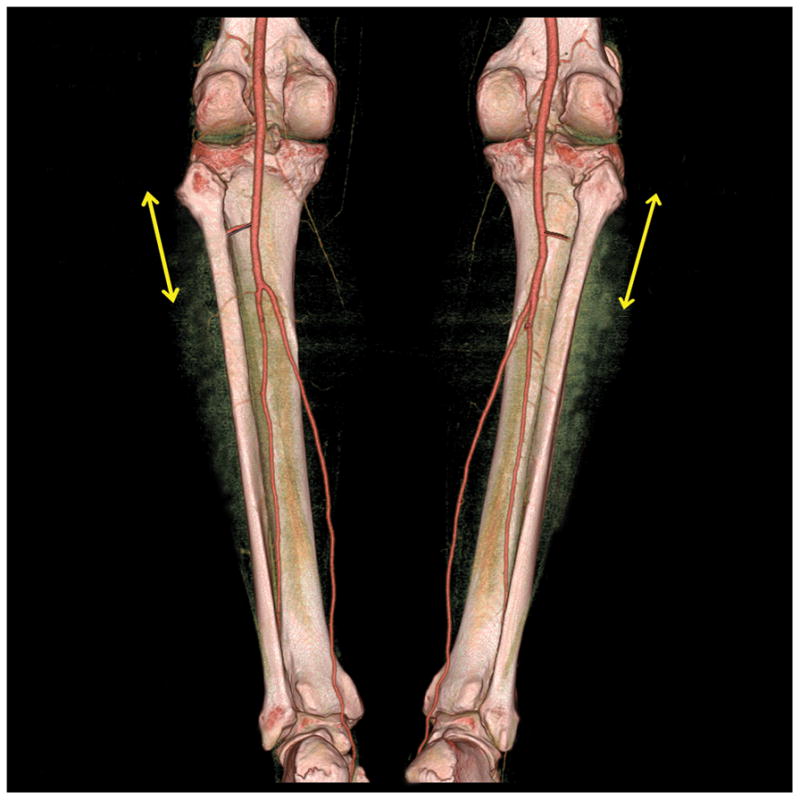
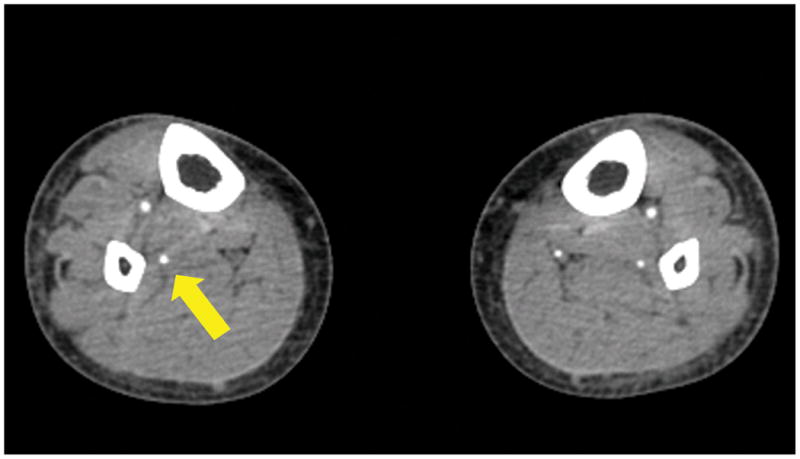
The authors studied a prospective cohort of 40 consecutive patients who underwent preoperative computed tomographic angiography mapping of the peroneal artery and its perforators and subsequent free fibula flap reconstruction of mandibular or maxillary defects. The authors compared their analysis of perforator anatomy, peroneal artery origin, and fibula length with intraoperative clinical findings.
Overall, computed tomographic angiography identified 94.9 percent of the cutaneous perforators found intraoperatively. Clinically, perforators were located an average of 8.7 mm from their predicted locations. The peroneal artery origin from the tibioperoneal trunk averaged 6.0 mm from its predicted location. The average length of the fibula differed from the predicted length by 8.0 mm. Computed tomographic angiography accurately predicted perforators as either septocutaneous or musculocutaneous 93.0 percent of the time. Perforator size was accurately predicted 66.7 percent of the time. Skin islands and osteotomies were modified in 25.0 percent of the cases on the basis of computed tomographic angiography findings. Two patients had hypoplastic posterior tibial arteries, prompting selection of the contralateral leg. There were no total flap or skin paddle losses.
Computed tomographic angiography accurately predicted the course and location of the peroneal artery and perforators; perforator size was less accurately estimated. Computed tomographic angiography provides valuable information to facilitate osteocutaneous fibula flap harvest.
在设计骨皮瓣游离腓骨时,由于计划不当、解剖异常或穿支不足,可能需要修改皮瓣设计、探查对侧肢体或增加皮瓣采集。作者研究了计算机断层血管造影术在骨皮瓣游离腓骨规划和执行中的预测能力。
作者研究了一组连续的 40 例患者,这些患者接受了术前腓动脉及其穿支的计算机断层血管造影图扫描,并随后进行游离腓骨瓣重建下颌或上颌缺损。作者将他们对穿支解剖、腓动脉起源和腓骨长度的分析与术中临床发现进行了比较。
总的来说,计算机断层血管造影术识别出了术中发现的 94.9%的皮穿支。临床上,穿支位于预测位置的平均距离为 8.7mm。胫腓干发自腓动脉的起点平均距离其预测位置 6.0mm。腓骨的平均长度与预测长度相差 8.0mm。计算机断层血管造影术准确地预测了 93.0%的穿支为皮肌穿支或皮血管支。穿支大小的预测准确率为 66.7%。根据计算机断层血管造影术的结果,有 25.0%的病例修改了皮岛和截骨术。有 2 例患者出现后胫腓动脉发育不良,促使选择对侧肢体。没有发生全部皮瓣或皮瓣失活。
计算机断层血管造影术能准确预测腓动脉和穿支的走行和位置;穿支大小的预测则不够准确。计算机断层血管造影术为游离腓骨骨皮瓣采集提供了有价值的信息。