Massachusetts General Hospital Cancer Center, Boston, USA.
N Engl J Med. 2012 Nov 1;367(18):1694-703. doi: 10.1056/NEJMoa1210093. Epub 2012 Sep 29.
Resistance to therapy with BRAF kinase inhibitors is associated with reactivation of the mitogen-activated protein kinase (MAPK) pathway. To address this problem, we conducted a phase 1 and 2 trial of combined treatment with dabrafenib, a selective BRAF inhibitor, and trametinib, a selective MAPK kinase (MEK) inhibitor.
In this open-label study involving 247 patients with metastatic melanoma and BRAF V600 mutations, we evaluated the pharmacokinetic activity and safety of oral dabrafenib (75 or 150 mg twice daily) and trametinib (1, 1.5, or 2 mg daily) in 85 patients and then randomly assigned 162 patients to receive combination therapy with dabrafenib (150 mg) plus trametinib (1 or 2 mg) or dabrafenib monotherapy. The primary end points were the incidence of cutaneous squamous-cell carcinoma, survival free of melanoma progression, and response. Secondary end points were overall survival and pharmacokinetic activity.
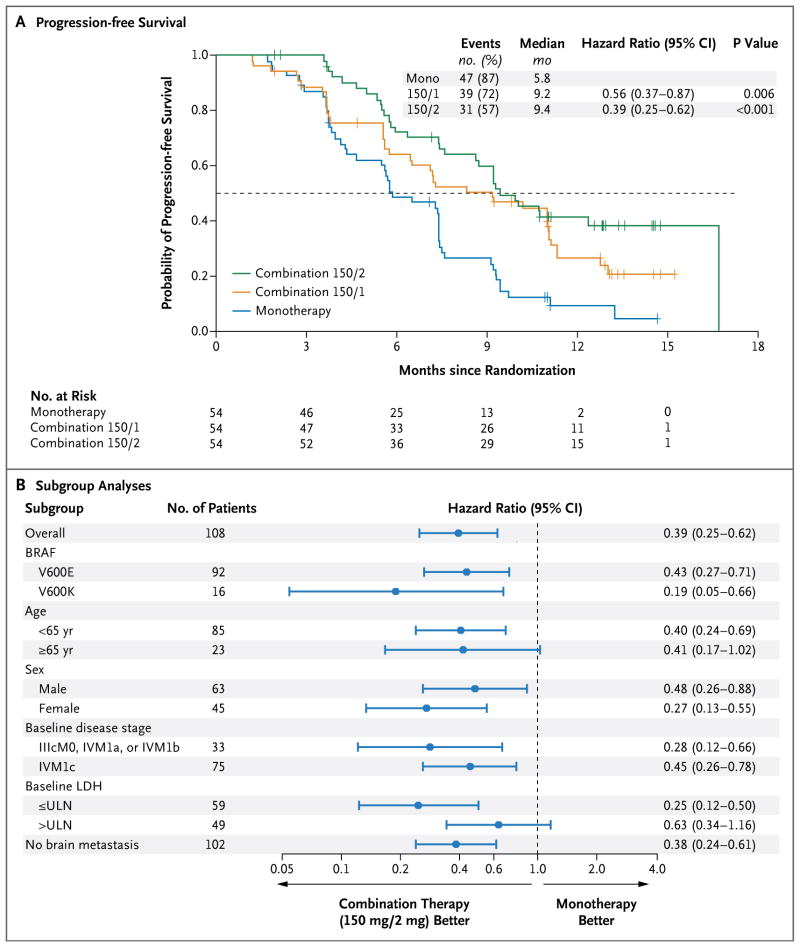
Dose-limiting toxic effects were infrequently observed in patients receiving combination therapy with 150 mg of dabrafenib and 2 mg of trametinib (combination 150/2). Cutaneous squamous-cell carcinoma was seen in 7% of patients receiving combination 150/2 and in 19% receiving monotherapy (P=0.09), whereas pyrexia was more common in the combination 150/2 group than in the monotherapy group (71% vs. 26%). Median progression-free survival in the combination 150/2 group was 9.4 months, as compared with 5.8 months in the monotherapy group (hazard ratio for progression or death, 0.39; 95% confidence interval, 0.25 to 0.62; P<0.001). The rate of complete or partial response with combination 150/2 therapy was 76%, as compared with 54% with monotherapy (P=0.03).
Dabrafenib and trametinib were safely combined at full monotherapy doses. The rate of pyrexia was increased with combination therapy, whereas the rate of proliferative skin lesions was nonsignificantly reduced. Progression-free survival was significantly improved. (Funded by GlaxoSmithKline; ClinicalTrials.gov number, NCT01072175.).
对 BRAF 激酶抑制剂治疗的耐药性与丝裂原活化蛋白激酶(MAPK)通路的再激活有关。为了解决这个问题,我们进行了一项 I/II 期试验,联合使用选择性 BRAF 抑制剂 dabrafenib 和选择性 MAPK 激酶(MEK)抑制剂 trametinib。
在这项涉及 247 例携带 BRAF V600 突变的转移性黑色素瘤患者的开放性研究中,我们评估了 85 例患者口服 dabrafenib(75 或 150mg,每日两次)和 trametinib(1、1.5 或 2mg,每日一次)的药代动力学活性和安全性,然后将 162 例患者随机分配接受 dabrafenib(150mg)加 trametinib(1 或 2mg)联合治疗或 dabrafenib 单药治疗。主要终点是皮肤鳞状细胞癌的发生率、无黑色素瘤进展的生存情况和反应。次要终点是总生存期和药代动力学活性。
接受 150mg dabrafenib 和 2mg trametinib 联合治疗的患者中,很少观察到剂量限制毒性作用(联合 150/2 组)。联合 150/2 组有 7%的患者出现皮肤鳞状细胞癌,而单药组有 19%(P=0.09),而联合 150/2 组发热更为常见(71%比 26%)。联合 150/2 组的中位无进展生存期为 9.4 个月,而单药组为 5.8 个月(进展或死亡的风险比为 0.39;95%置信区间为 0.25 至 0.62;P<0.001)。联合 150/2 治疗的完全或部分缓解率为 76%,而单药组为 54%(P=0.03)。
dabrafenib 和 trametinib 在全剂量单药治疗时安全联合使用。联合治疗组发热率增加,而增殖性皮肤病变率无显著降低。无进展生存期显著改善。(由葛兰素史克公司资助;ClinicalTrials.gov 编号,NCT01072175。)