Division of Rheumatology, NYU Hospital for Joint Diseases, New York, New York USA.
BMJ Open. 2012 Oct 3;2(5). doi: 10.1136/bmjopen-2012-001117. Print 2012.
The new 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria for rheumatoid arthritis (RA) have been designed to classify early onset RA, but has not been studied to identify RA in patients with arthritis seen in routine clinical care where correct 'classification' of patients, when they are not selected for having RA would be important.
Prospective, consecutive patients cohort.
Outpatient clinic of a university rheumatology centre.
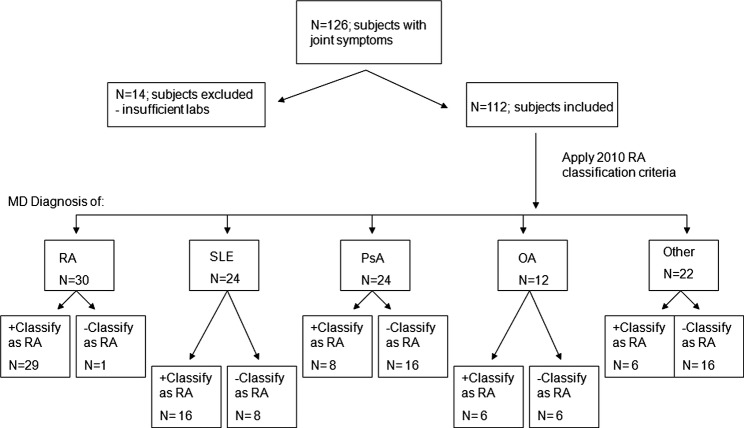
A total of 126 patients with joint symptoms were consecutively recruited.
The ACR/EULAR RA criteria were applied, with questions followed by a targeted musculoskeletal exam. The gold standard for the diagnosis of RA was the primary rheumatologist's diagnosis.
Number of patients with non-RA diagnosis who were classified as having RA by the new classification criteria.
The sensitivity and specificity of the 2010 criteria in classifying RA were 97% and 55%, respectively, compared with the 1987 RA criteria which were 93% and 76%, respectively. The 2010 criteria as applied to this group of patients had a poorer positive predictive (44% vs 61%) and a similar negative predictive value (98% vs 97%) compared with the 1987 criteria. More specifically, 66.7% of systemic lupus erythematosus patients, 50% of osteoarthritis, 37.5% of psoriatic arthritis and 27.2% of others fulfilled the new criteria and could have been classified as RA.
In this, we believe, the first study to examine the new 2010 ACR/EULAR RA criteria among consecutive patients seen in routine care, we found the criteria to have low specificity, and therefore incorrectly label those as having RA when, in fact, they may have a different type of inflammatory arthritis. Physicians need to be aware of this when applying the new criteria for classifying their patients for any purpose.
新的 2010 年美国风湿病学会/欧洲抗风湿病联盟(ACR/EULAR)类风湿关节炎(RA)标准旨在分类早期发病的 RA,但尚未研究用于识别在常规临床护理中出现关节炎的患者中的 RA,在这种情况下,正确“分类”患者非常重要,因为这些患者并非都因 RA 而被选择。
前瞻性、连续患者队列。
大学风湿病中心的门诊诊所。
共连续招募了 126 名有关节症状的患者。
应用 ACR/EULAR RA 标准,问题后面跟着针对性的肌肉骨骼检查。RA 的金标准是初级风湿病医生的诊断。
通过新分类标准将非 RA 诊断的患者分类为 RA 的患者数量。
与 1987 年 RA 标准的敏感性和特异性分别为 93%和 76%相比,2010 年标准的敏感性和特异性分别为 97%和 55%。在应用于该组患者的 2010 年标准中,阳性预测值(44%比 61%)和阴性预测值(98%比 97%)均较差。更具体地说,66.7%的系统性红斑狼疮患者、50%的骨关节炎患者、37.5%的银屑病关节炎患者和 27.2%的其他疾病患者符合新的标准,可能被归类为 RA。
在这项我们认为是首次在常规护理中连续观察患者的新的 2010 年 ACR/EULAR RA 标准的研究中,我们发现该标准特异性较低,因此错误地将那些患有 RA 的患者归类为 RA,而实际上他们可能患有不同类型的炎症性关节炎。当医生出于任何目的应用新标准对患者进行分类时,需要注意这一点。