Department of Pediatrics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand.
BMC Gastroenterol. 2012 Oct 15;12:141. doi: 10.1186/1471-230X-12-141.
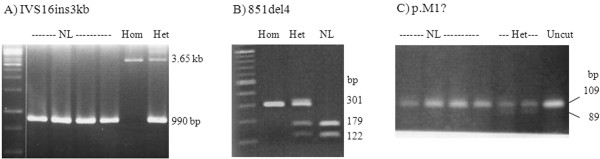
The most common causes of cholestatic jaundice are biliary atresia and idiopathic neonatal hepatitis (INH). Specific disorders underlying INH, such as various infectious and metabolic causes, including neonatal intrahepatic cholestasis caused by citrin deficiency (NICCD) especially, in East Asian populations are increasingly being identified. Since most NICCD infants recovered from liver disease by 1 year of age, they often are misdiagnosed with INH, leading to difficulty in determining the true prevalence of NICCD. Mutation(s) of human SLC25A13 gene encoding a mitochondrial aspartate/glutamate carrier isoform 2 (AGC2), can lead to AGC2 deficiency, resulting in NICCD and an adult-onset fatal disease namely citrullinemia type II (CTLN2). To study the prevalence of NICCD and SLC25A13 mutations in Thai infants, and to compare manifestations of NICCD and non-NICCD, infants with idiopathic cholestatic jaundice or INH were enrolled. Clinical and biochemical data were reviewed. Urine organic acid and plasma amino acids profiles were analyzed. PCR-sequencing of all 18 exons of SLC25A13 and gap PCR for the mutations IVS16ins3kb and Ex16+74_IVS17-32del516 were performed. mRNA were analyzed in selected cases with possible splicing error.
Five out of 39 (12.8%) unrelated infants enrolled in the study were found to have NICCD, of which three had homozygous 851del4 (GTATdel) and two compound heterozygous 851del4/IVS16ins3kb and 851del4/1638ins23, respectively. Two missense mutations (p.M1? and p.R605Q) of unknown functional significance were identified. At the initial presentation, NICCD patients had higher levels of alkaline phosphatase (ALP) and alpha-fetoprotein (AFP) and lower level of alanine aminotransferase (ALT) than those in non-NICCD patients (p< 0.05). NICCD patients showed higher citrulline level and threonine/serine ratio than non-NICCD infants (p< 0.05). Fatty liver was found in 2 NICCD patients. Jaundice resolved in all NICCD and in 87.5% of non-NICCD infants at the median age of 9.5 and 4.0 months, respectively.
NICCD should be considered in infants with idiopathic cholestasis. The preliminary estimated prevalence of NICCD was calculated to be 1/48,228 with carrier rate of 1/110 among Thai infants. However, this number may be underestimated and required further analysis with mutation screening in larger control population to establish the true prevalence of NICCD and AGC2 deficiency.
胆汁淤积性黄疸最常见的原因是胆道闭锁和特发性新生儿肝炎(INH)。INH 所涉及的特定疾病,如各种感染性和代谢性疾病,包括 citrin 缺乏症(NICCD)引起的新生儿肝内胆汁淤积症,在东亚人群中越来越多地被发现。由于大多数 NICCD 婴儿在 1 岁前从肝脏疾病中康复,因此它们经常被误诊为 INH,这导致难以确定 NICCD 的真实患病率。人类 SLC25A13 基因的突变可导致天冬氨酸/谷氨酸载体同工型 2(AGC2)的缺乏,从而导致 NICCD 和成年致命疾病即瓜氨酸血症 II 型(CTLN2)。为了研究 NICCD 和 SLC25A13 突变在泰国婴儿中的流行情况,并比较 NICCD 和非 NICCD 的表现,我们招募了患有特发性胆汁淤积性黄疸或 INH 的婴儿。回顾临床和生化数据。分析尿液有机酸和血浆氨基酸谱。对 SLC25A13 的所有 18 个外显子进行 PCR 测序,并对突变 IVS16ins3kb 和 Ex16+74_IVS17-32del516 进行 gap-PCR。对可能存在剪接错误的选定病例进行 mRNA 分析。
在研究中纳入的 39 名无血缘关系的婴儿中,有 5 名(12.8%)被发现患有 NICCD,其中 3 名纯合 851del4(GTATdel),2 名复合杂合 851del4/IVS16ins3kb 和 851del4/1638ins23。鉴定出两个功能未知的错义突变(p.M1?和 p.R605Q)。在初始表现时,NICCD 患者的碱性磷酸酶(ALP)和甲胎蛋白(AFP)水平较高,丙氨酸氨基转移酶(ALT)水平较低(p<0.05)。NICCD 患者的瓜氨酸水平和苏氨酸/丝氨酸比值高于非 NICCD 婴儿(p<0.05)。2 名 NICCD 患者有脂肪肝。所有 NICCD 患者和 87.5%的非 NICCD 患者的黄疸在中位年龄为 9.5 和 4.0 个月时消退。
应考虑 NICCD 作为特发性胆汁淤积症的婴儿。初步估计 NICCD 的患病率为 1/48228,泰国婴儿的携带者率为 1/110。然而,这个数字可能被低估了,需要在更大的对照人群中进行突变筛查的进一步分析,以确定 NICCD 和 AGC2 缺乏症的真实患病率。