The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA.
Gynecol Oncol. 2013 Feb;128(2):155-9. doi: 10.1016/j.ygyno.2012.11.034. Epub 2012 Nov 29.
To determine which patients with near midline lesions may safely undergo unilateral groin dissection based on clinical exam and lymphoscintigraphy (LSG) results.
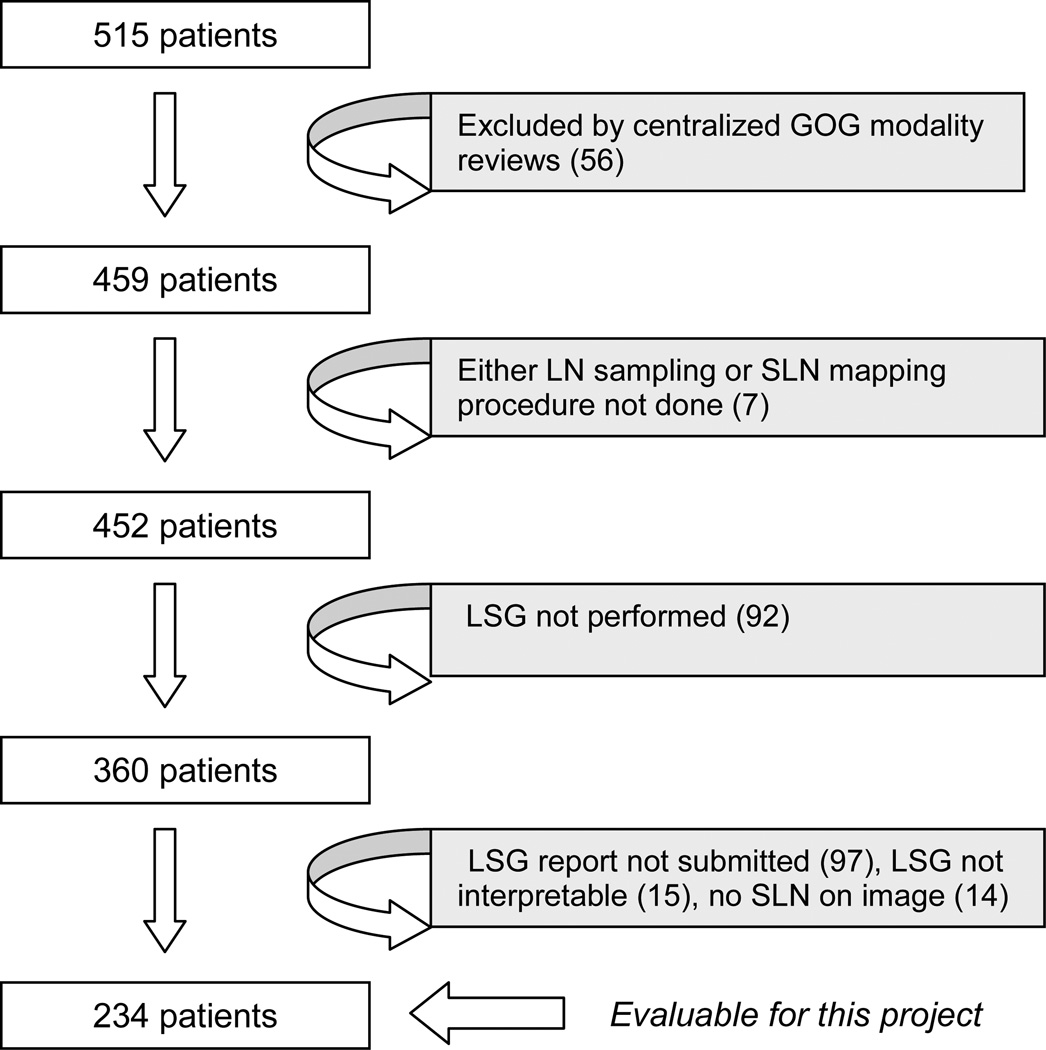
Patients participating in GOG-173 underwent sentinel lymph node (SLN) localization with blue dye, and radiocolloid with optional LSG before definitive inguinal-femoral lymphadenectomy (LND). This analysis interrogates the reliability of LSG alone relative to primary tumor location in those patients who had an interpretable LSG and at least one SLN identified. Primary tumor location was categorized as lateral (>2cm from midline), midline, or lateral ambiguous (LA) if located within 2cm, but not involving the midline.
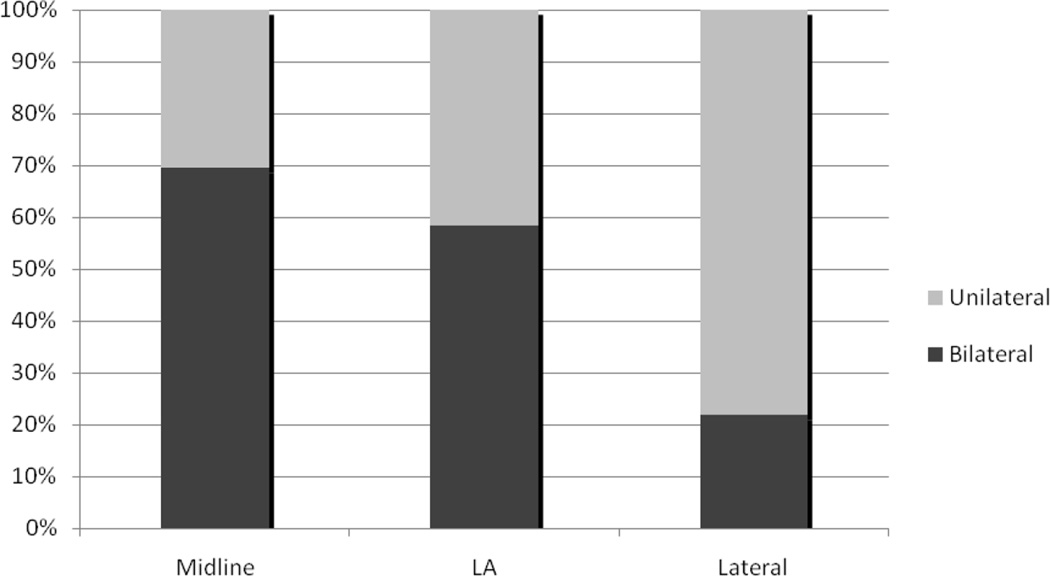
Two-hundred-thirty-four patients met eligibility criteria. Sixty-four had lateral lesions, and underwent unilateral LND. All patients with LA (N=65) and midline (N=105) tumors underwent bilateral LND. Bilateral drainage by LSG was identified in 14/64 (22%) patients with lateral tumors, 38/65 (58%) with LA tumors and in 73/105 (70%) with midline tumors. At mapping, no SLNs were found in contralateral groins among those patients with LA and midline tumors who had unilateral-only LSGs. However, in these patients groin metastases were found in 4/32 patients with midline tumors undergoing contralateral dissection; none were found in 27 patients with LA tumors.
The likelihood of detectable bilateral drainage using preoperative LSG decreases as a function of distance from midline. Patients with LA primaries and unilateral drainage on LSG may safely undergo unilateral SLN.
根据临床检查和淋巴闪烁显像术(LSG)的结果,确定哪些中线附近病变的患者可以安全地进行单侧腹股沟解剖。
参与 GOG-173 的患者在接受明确的腹股沟-股部淋巴结清扫术(LND)之前,通过蓝染剂和放射性胶体进行前哨淋巴结(SLN)定位,并选择性进行 LSG。本分析通过 LSG 与原发性肿瘤位置的相关性来评估 LSG 的可靠性,这些患者具有可解释的 LSG 且至少有一个 SLN 被识别。原发性肿瘤位置分为外侧(距中线>2cm)、中线或外侧不确定(LA),如果位于 2cm 以内,但不涉及中线。
234 名患者符合入选标准。64 名患者有外侧病变,行单侧 LND。所有 LA(N=65)和中线(N=105)肿瘤患者均行双侧 LND。在 64 名外侧肿瘤患者中,有 14 名(22%)患者出现 LSG 双侧引流,38 名(58%)LA 肿瘤患者和 73 名(70%)中线肿瘤患者出现 LSG 双侧引流。在 SLN 定位时,LA 和中线肿瘤患者中,那些仅进行单侧 LSG 的患者对侧腹股沟中未发现 SLN。然而,在这些患者中,有 4 名中线肿瘤患者在接受对侧解剖时发现腹股沟转移,而 27 名 LA 肿瘤患者未发现腹股沟转移。
术前 LSG 检测到双侧引流的可能性随距离中线的增加而降低。LA 原发肿瘤和 LSG 单侧引流的患者可安全地进行单侧 SLN。