Bellato Enrico, Marini Eleonora, Castoldi Filippo, Barbasetti Nicola, Mattei Lorenzo, Bonasia Davide Edoardo, Blonna Davide
Department of Orthopedics and Traumatology, Mauriziano Umberto I Hospital, University of Turin Medical School, Largo Turati 62,10128 Turin, Italy [corrected].
Pain Res Treat. 2012;2012:426130. doi: 10.1155/2012/426130. Epub 2012 Nov 4.
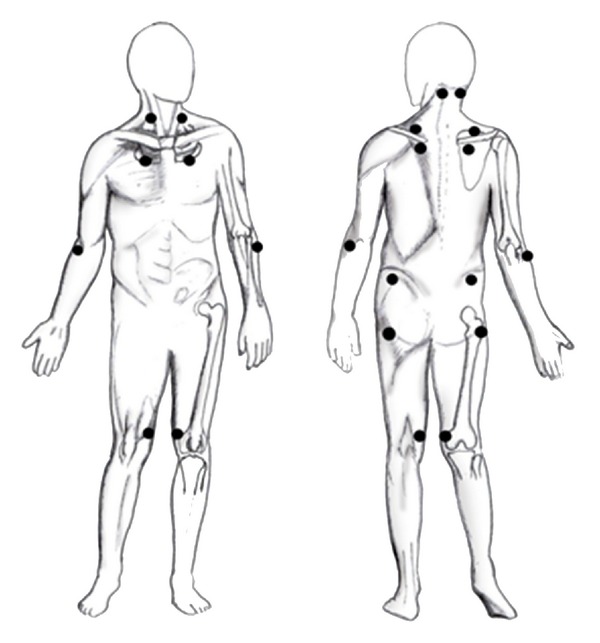
Fibromyalgia syndrome is mainly characterized by pain, fatigue, and sleep disruption. The etiology of fibromyalgia is still unclear: if central sensitization is considered to be the main mechanism involved, then many other factors, genetic, immunological, and hormonal, may play an important role. The diagnosis is typically clinical (there are no laboratory abnormalities) and the physician must concentrate on pain and on its features. Additional symptoms (e.g., Raynaud's phenomenon, irritable bowel disease, and heat and cold intolerance) can be associated with this condition. A careful differential diagnosis is mandatory: fibromyalgia is not a diagnosis of exclusion. Since 1990, diagnosis has been principally based on the two major diagnostic criteria defined by the ACR. Recently, new criteria have been proposed. The main goals of the treatment are to alleviate pain, increase restorative sleep, and improve physical function. A multidisciplinary approach is optimal. While most nonsteroidal anti-inflammatory drugs and opioids have limited benefit, an important role is played by antidepressants and neuromodulating antiepileptics: currently duloxetine (NNT for a 30% pain reduction 7.2), milnacipran (NNT 19), and pregabalin (NNT 8.6) are the only drugs approved by the US Food and Drug Administration for the treatment of fibromyalgia. In addition, nonpharmacological treatments should be associated with drug therapy.
纤维肌痛综合征主要表现为疼痛、疲劳和睡眠障碍。纤维肌痛的病因仍不明确:如果认为中枢敏化是主要涉及的机制,那么许多其他因素,如遗传、免疫和激素因素,可能发挥重要作用。诊断通常基于临床(无实验室异常),医生必须关注疼痛及其特征。其他症状(如雷诺现象、肠易激综合征以及冷热不耐受)可能与该病症相关。必须进行仔细的鉴别诊断:纤维肌痛并非排除性诊断。自1990年以来,诊断主要基于美国风湿病学会(ACR)定义的两大诊断标准。最近,又提出了新的标准。治疗的主要目标是减轻疼痛、增加恢复性睡眠并改善身体功能。多学科方法是最佳选择。虽然大多数非甾体抗炎药和阿片类药物的益处有限,但抗抑郁药和神经调节性抗癫痫药发挥着重要作用:目前,度洛西汀(使疼痛减轻30%的所需治疗人数为7.2)、米那普明(所需治疗人数为19)和普瑞巴林(所需治疗人数为8.6)是美国食品药品监督管理局批准用于治疗纤维肌痛的仅有的药物。此外,非药物治疗应与药物治疗相结合。