Narlidere Community Health Center, Ministry of Health of Turkey, Izmir, Narlıdere, Turkey.
Int J Equity Health. 2012 Dec 5;11:73. doi: 10.1186/1475-9276-11-73.
This study aimed to measure socioeconomic inequalities in Self Assessed Health (SAH) and evaluate the determinants of such inequalities in terms of their contributions amongst the Turkish population.
We used data from the Turkish part of World Health Survey 2003 with 10,287 respondents over 18 years old. Concentration index (CI) of SAH was calculated as a measure of socioeconomic inequalities in health, and contributions of each determinant to inequality were evaluated using a decomposition method.
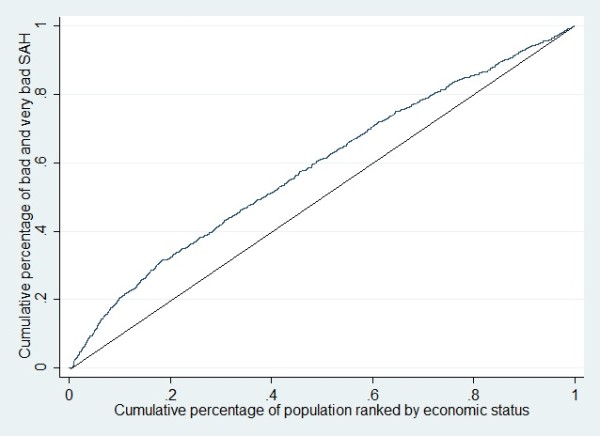
In total 952 participants (9.3%) rated their health status as either bad or very bad. The CI for SAH was -0.15, suggesting that suboptimal SAH was reported more by those categorised as poor. The multiple logistic regression results indicated that having secondary, primary or less than primary school education, not being married and being in the lowest wealth quintile, significantly increased the risk of having poor SAH. The largest contributions to inequality were attributed to education level (70.7%), household economic status (9.7%) and geographical area lived in (8.4%).
The findings indicate that socioeconomic inequalities measured by SAH are apparent amongst the Turkish population. Education and household wealth were the greatest contributing factors to SAH inequality. These inequalities need to be explicitly addressed and vulnerable subgroups should be targeted to reduce the socioeconomic disparities.
本研究旨在衡量土耳其人群中自我评估健康(SAH)的社会经济不平等,并评估这些不平等的决定因素,以确定其对不平等的贡献。
我们使用了 2003 年世界卫生调查土耳其部分的数据,其中包括 10287 名 18 岁以上的受访者。采用集中指数(CI)来衡量健康方面的社会经济不平等,并使用分解方法评估每个决定因素对不平等的贡献。
共有 952 名参与者(9.3%)将其健康状况评为差或非常差。SAH 的 CI 为-0.15,表明较差的 SAH 报告更多的是被归类为贫困的人群。多因素逻辑回归结果表明,接受中等、初等或低于初等教育、未婚和处于最低财富五分位数的人,其健康状况差的风险显著增加。对不平等的最大贡献归因于教育水平(70.7%)、家庭经济状况(9.7%)和居住地区(8.4%)。
研究结果表明,土耳其人群中存在以 SAH 衡量的社会经济不平等。教育和家庭财富是导致 SAH 不平等的最大因素。这些不平等需要明确解决,应该针对弱势群体采取措施,以减少社会经济差距。