Neonatal Intensive Care Unit, Department of Clinical Science and Comunity Health, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, University of Milan, Milan, Italy.
PLoS One. 2012;7(12):e51166. doi: 10.1371/journal.pone.0051166. Epub 2012 Dec 5.
Prevention of postnatal growth restriction of very preterm infants still represents a challenge for neonatologists. As standard feeding regimens have proven to be inadequate. Improved feeding strategies are needed to promote growth. Aim of the present study was to evaluate whether a set of nutritional strategies could limit the postnatal growth restriction of a cohort of preterm infants.
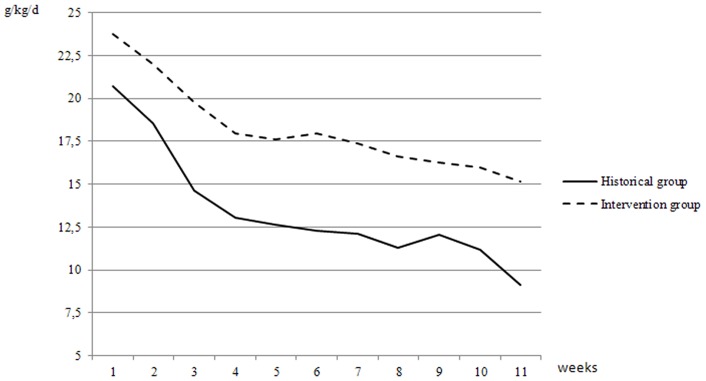
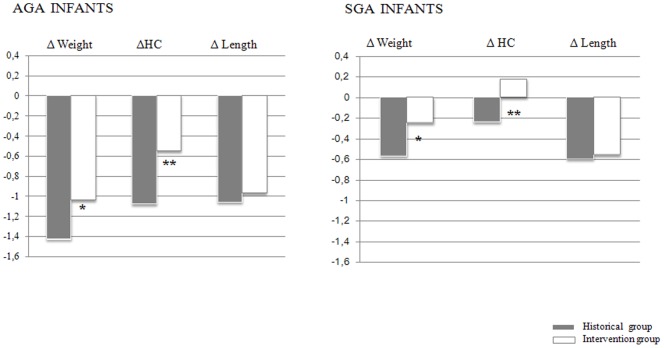
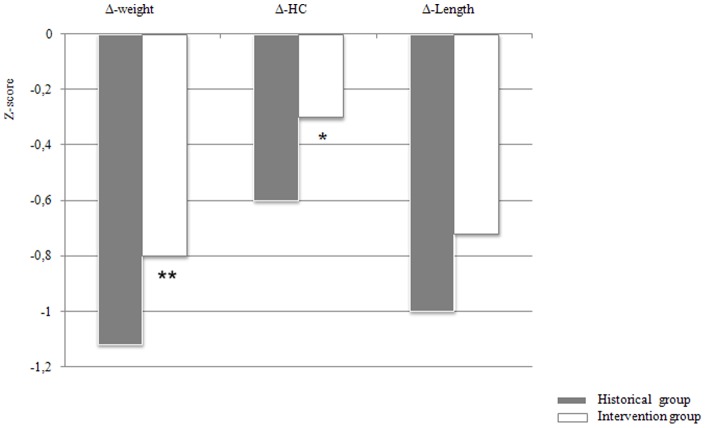
METHODOLOGY/PRINCIPAL FINDINGS: We performed a prospective non randomized interventional cohort study. Growth and body composition were assessed in 102 very low birth weight infants after the introduction of a set of nutritional practice changes. 69 very low birth weight infants who had received nutrition according to the standard nutritional feeding strategy served as a historical control group. Weight was assessed daily, length and head circumference weekly. Body composition at term corrected age was assessed using an air displacement plethysmography system. The cumulative parenteral energy and protein intakes during the first 7 days of life were higher in the intervention group than in the historical group (530 ± 81 vs 300 ± 93 kcal/kg, p<0.001 and 21 ± 2.9 vs 15 ± 3.2 g/kg, p<0.01). During weaning from parenteral nutrition, the intervention group received higher parental/enteral energy and protein intakes than the historical control group (1380 ± 58 vs 1090 ± 70 kcal/kg; 52.6 ± 7 vs 42.3 ± 10 g/kg, p<0.01). Enteral energy (kcal/kg/d) and protein (g/kg/d) intakes in the intervention group were higher than in the historical group (130 ± 11 vs 100 ± 13; 3.5 ± 0.5 vs 2.2 ± 0.6, p<0.01). The negative changes in z score from birth to discharge for weight and head circumference were significantly lower in the intervention group as compared to the historical group. No difference in fat mass percentage between the intervention and the historical groups was found.
The optimization and the individualization of nutritional intervention promote postnatal growth of preterm infants without any effect on percentage of fat mass.
预防极早产儿的产后生长受限仍然是新生儿科医生面临的挑战。由于标准喂养方案已被证明是不够的,因此需要改进喂养策略来促进生长。本研究旨在评估一组营养策略是否可以限制早产儿队列的产后生长受限。
方法/主要发现:我们进行了一项前瞻性非随机干预性队列研究。在引入一组营养实践改变后,评估了 102 名极低出生体重儿的生长和身体成分。 69 名接受标准营养喂养策略营养的极低出生体重儿作为历史对照组。每天评估体重,每周评估身长和头围。在纠正胎龄时使用空气置换体描仪系统评估身体成分。干预组在生命的前 7 天内接受的累积肠外能量和蛋白质摄入量高于历史组(530±81 与 300±93 千卡/公斤,p<0.001 和 21±2.9 与 15±3.2 克/公斤,p<0.01)。在从肠外营养过渡期间,干预组接受的肠外/肠内能量和蛋白质摄入量高于历史对照组(1380±58 与 1090±70 千卡/公斤;52.6±7 与 42.3±10 克/公斤,p<0.01)。干预组的肠内能量(千卡/公斤/天)和蛋白质(克/公斤/天)摄入量高于历史组(130±11 与 100±13;3.5±0.5 与 2.2±0.6,p<0.01)。与历史组相比,干预组出生至出院时体重和头围 z 评分的负变化明显更低。干预组和历史组之间的脂肪百分比没有差异。
营养干预的优化和个体化促进了早产儿的产后生长,而对脂肪百分比没有影响。