Department of Pediatrics, University of California at San Diego, San Diego, California 92013, USA.
N Engl J Med. 2012 Dec 27;367(26):2495-504. doi: 10.1056/NEJMoa1208506.
Previous results from our trial of early treatment with continuous positive airway pressure (CPAP) versus early surfactant treatment in infants showed no significant difference in the outcome of death or bronchopulmonary dysplasia. A lower (vs. higher) target range of oxygen saturation was associated with a lower rate of severe retinopathy but higher mortality. We now report longer-term results from our prespecified hypotheses.
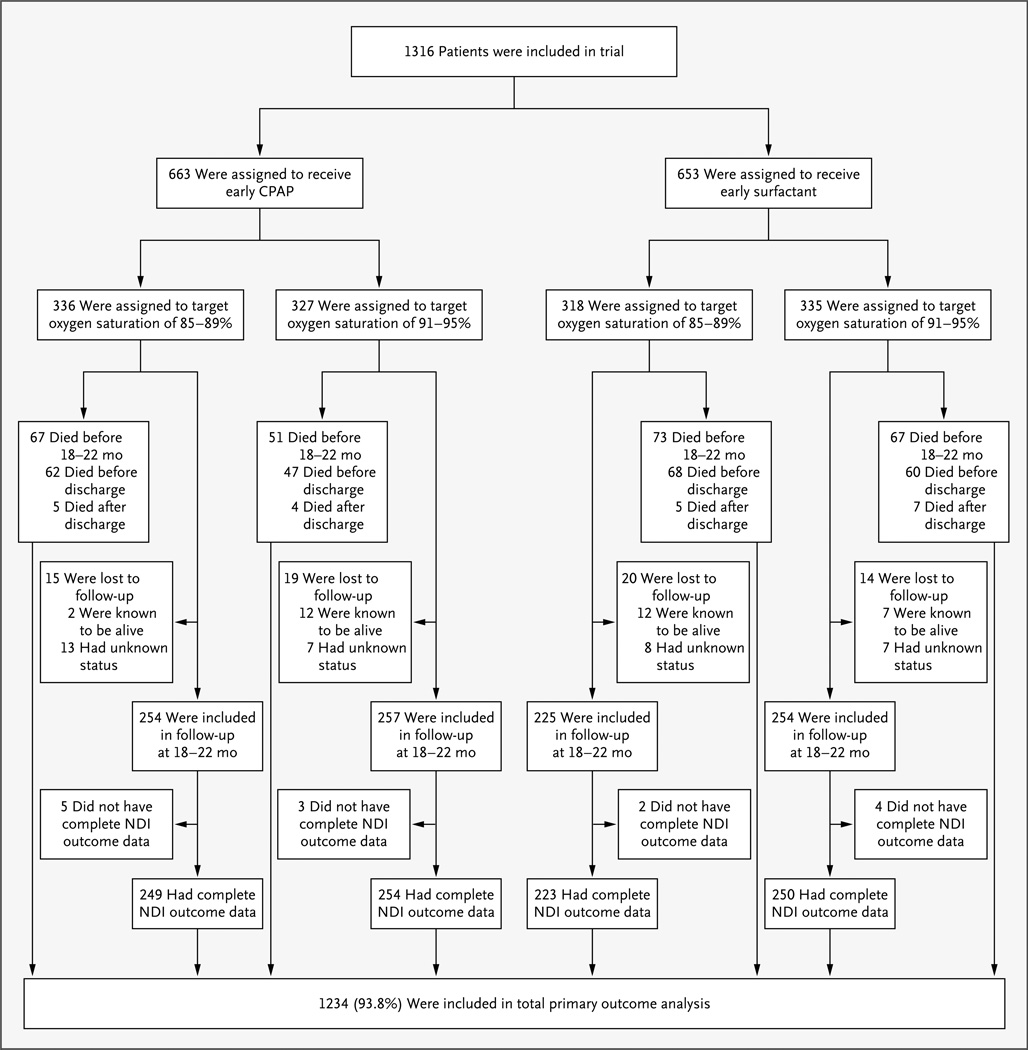
Using a 2-by-2 factorial design, we randomly assigned infants born between 24 weeks 0 days and 27 weeks 6 days of gestation to early CPAP with a limited ventilation strategy or early surfactant administration and to lower or higher target ranges of oxygen saturation (85 to 89% or 91 to 95%). The primary composite outcome for the longer-term analysis was death before assessment at 18 to 22 months or neurodevelopmental impairment at 18 to 22 months of corrected age.
The primary outcome was determined for 1234 of 1316 enrolled infants (93.8%); 990 of the 1058 surviving infants (93.6%) were evaluated at 18 to 22 months of corrected age. Death or neurodevelopmental impairment occurred in 27.9% of the infants in the CPAP group (173 of 621 infants), versus 29.9% of those in the surfactant group (183 of 613) (relative risk, 0.93; 95% confidence interval [CI], 0.78 to 1.10; P=0.38), and in 30.2% of the infants in the lower-oxygen-saturation group (185 of 612), versus 27.5% of those in the higher-oxygen-saturation group (171 of 622) (relative risk, 1.12; 95% CI, 0.94 to 1.32; P=0.21). Mortality was increased with the lower-oxygen-saturation target (22.1%, vs. 18.2% with the higher-oxygen-saturation target; relative risk, 1.25; 95% CI, 1.00 to 1.55; P=0.046).
We found no significant differences in the composite outcome of death or neurodevelopmental impairment among extremely premature infants randomly assigned to early CPAP or early surfactant administration and to a lower or higher target range of oxygen saturation. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Heart, Lung, and Blood Institute; SUPPORT ClinicalTrials.gov number, NCT00233324.).
我们之前进行的一项关于早期持续气道正压通气(CPAP)与早期表面活性剂治疗早产儿的试验结果显示,在死亡或支气管肺发育不良的结局方面,两种治疗方法没有显著差异。较低(而非较高)的目标血氧饱和度范围与较低的严重视网膜病变发生率相关,但与较高的死亡率相关。我们现在报告了我们预先设定的假设的长期结果。
采用 2×2 析因设计,我们将 24 周零 0 天至 27 周零 6 天之间出生的婴儿随机分为早期 CPAP 联合有限通气策略组或早期表面活性剂给药组,以及较低(85%89%)或较高(91%95%)目标血氧饱和度范围组。长期分析的主要复合结局是在 18 至 22 个月时评估前死亡或 18 至 22 个月时校正年龄的神经发育障碍。
1316 名入组婴儿中,有 1234 名(93.8%)确定了主要结局;在 1058 名存活婴儿中,有 990 名(93.6%)在 18 至 22 个月时校正年龄接受了评估。CPAP 组中 27.9%(621 名婴儿中的 173 名)和表面活性剂组中 29.9%(613 名婴儿中的 183 名)的婴儿发生死亡或神经发育障碍(相对风险,0.93;95%置信区间[CI],0.78 至 1.10;P=0.38),低氧饱和度组中 30.2%(612 名婴儿中的 185 名)和高氧饱和度组中 27.5%(622 名婴儿中的 171 名)的婴儿发生死亡或神经发育障碍(相对风险,1.12;95%CI,0.94 至 1.32;P=0.21)。较低的氧饱和度目标与死亡率增加相关(22.1%,与较高的氧饱和度目标相比为 18.2%;相对风险,1.25;95%CI,1.00 至 1.55;P=0.046)。
我们发现,随机分配接受早期 CPAP 或早期表面活性剂治疗以及较低或较高目标血氧饱和度范围的极早产儿在死亡或神经发育障碍的复合结局方面没有显著差异。(由美国国立儿童健康与人类发育研究所和美国国家心肺血液研究所资助;SUPPORT 临床试验.gov 编号,NCT00233324。)