Infectious Diseases Institute, Makerere College of Health Sciences, Kampala, Uganda.
PLoS One. 2012;7(12):e51631. doi: 10.1371/journal.pone.0051631. Epub 2012 Dec 17.
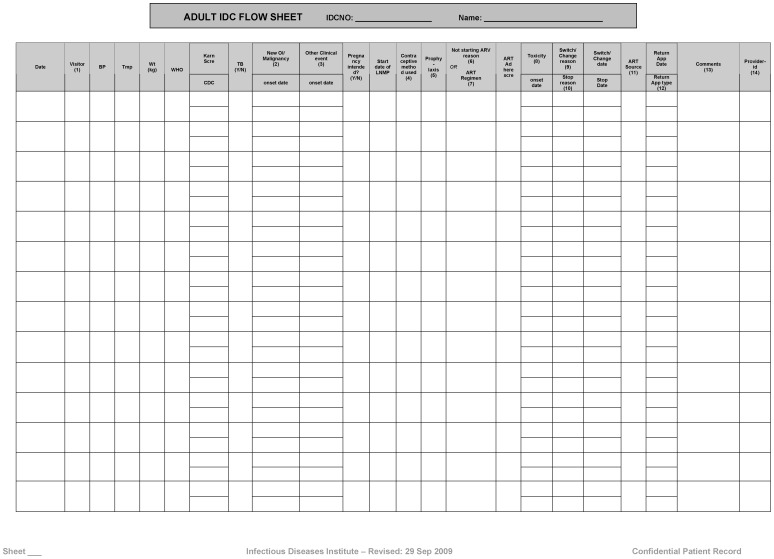
Starting in June 2010 the Infectious Diseases Institute (IDI) clinic (a large urban HIV out-patient facility) switched to provider-based Electronic Medical Records (EMR) from paper EMR entered in the database by data-entry clerks. Standardized clinics forms were eliminated but providers still fill free text clinical notes in physical patients' files. The objective of this study was to compare the rate of errors in the database before and after the introduction of the provider-based EMR.
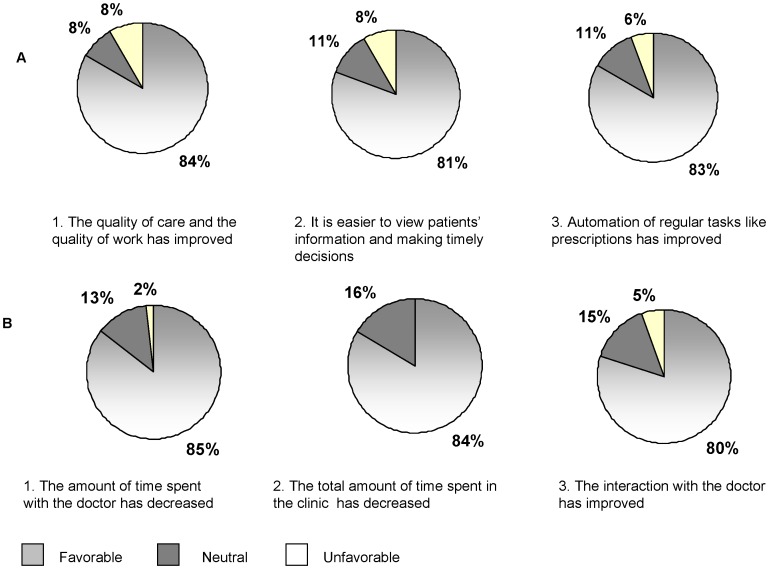
Data in the database pre and post provider-based EMR was compared with the information in the patients' files and classified as correct, incorrect, and missing. We calculated the proportion of incorrect, missing and total error for key variables (toxicities, opportunistic infections, reasons for treatment change and interruption). Proportions of total errors were compared using chi-square test. A survey of the users of the EMR was also conducted. We compared data from 2,382 visits (from 100 individuals) of a retrospective validation conducted in 2007 with 34,957 visits (from 10,920 individuals) of a prospective validation conducted in April-August 2011. The total proportion of errors decreased from 66.5% in 2007 to 2.1% in 2011 for opportunistic infections, from 51.9% to 3.5% for ART toxicity, from 82.8% to 12.5% for reasons for ART interruption and from 94.1% to 0.9% for reasons for ART switch (all P<0.0001). The survey showed that 83% of the providers agreed that provider-based EMR led to improvement of clinical care, 80% reported improved access to patients' records, and 80% appreciated the automation of providers' tasks.
The introduction of provider-based EMR improved the quality of data collected with a significant reduction in missing and incorrect information. The majority of providers and clients expressed satisfaction with the new system. We recommend the use of provider-based EMR in large HIV programs in Sub-Saharan Africa.
自 2010 年 6 月起,传染病研究所(IDI)门诊(一个大型城市艾滋病门诊)从由数据录入员输入数据库的纸质电子病历转为基于提供者的电子病历(EMR)。虽然标准化的诊所表格被取消了,但医生仍在患者的纸质病历中填写自由文本的临床记录。本研究的目的是比较引入基于提供者的 EMR 前后数据库中的错误率。
将基于提供者的 EMR 前后数据库中的数据与患者档案中的信息进行比较,并将其分类为正确、错误和缺失。我们计算了关键变量(毒性、机会性感染、治疗改变和中断的原因)的错误、缺失和总错误的比例。使用卡方检验比较总错误的比例。还对 EMR 的使用者进行了调查。我们比较了 2007 年进行的回顾性验证中的 2382 次就诊(来自 100 名个体)的数据和 2011 年 4 月至 8 月进行的前瞻性验证中的 34957 次就诊(来自 10920 名个体)的数据。机会性感染的总错误比例从 2007 年的 66.5%下降到 2011 年的 2.1%,ART 毒性从 51.9%下降到 3.5%,ART 中断的原因从 82.8%下降到 12.5%,ART 转换的原因从 94.1%下降到 0.9%(均 P<0.0001)。调查显示,83%的提供者认为基于提供者的 EMR 提高了临床护理质量,80%的提供者报告说更容易获得患者记录,80%的提供者赞赏提供者任务的自动化。
引入基于提供者的 EMR 提高了数据的质量,显著减少了缺失和错误信息。大多数提供者和患者对新系统表示满意。我们建议在撒哈拉以南非洲的大型艾滋病毒规划中使用基于提供者的 EMR。