Department of Surgery, Stony Brook University Medical Center, Stony Brook, NY, USA.
J Am Heart Assoc. 2012 Dec;1(6):e005652. doi: 10.1161/JAHA.112.005652. Epub 2012 Dec 19.
In situ cellular reprogramming offers the possibility of regenerating functional cardiomyocytes directly from scar fibroblasts, obviating the challenges of cell implantation. We hypothesized that pretreating scar with gene transfer of the angiogenic vascular endothelial growth factor (VEGF) would enhance the efficacy of this strategy.
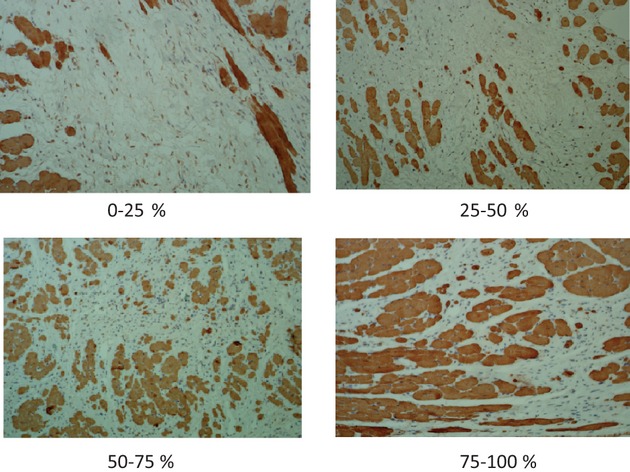
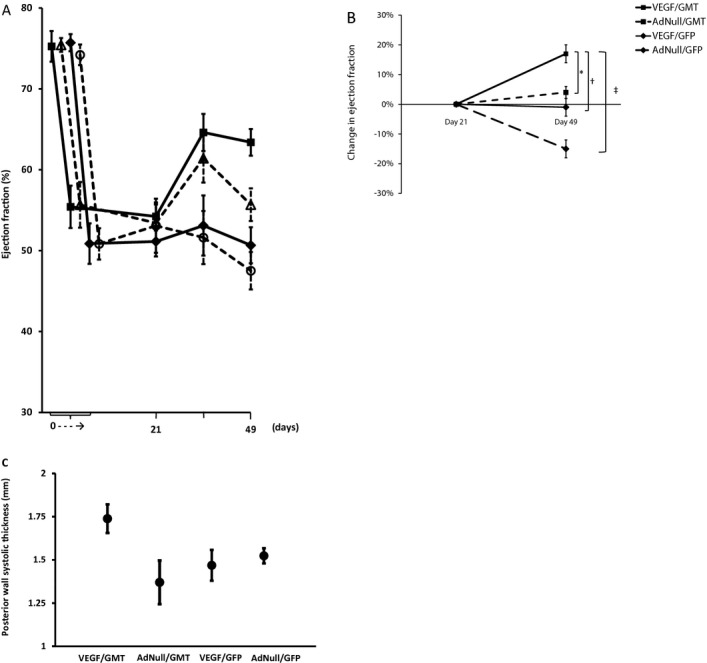
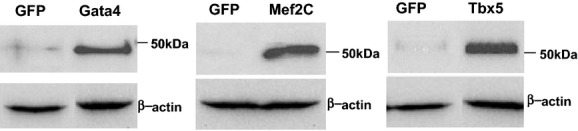
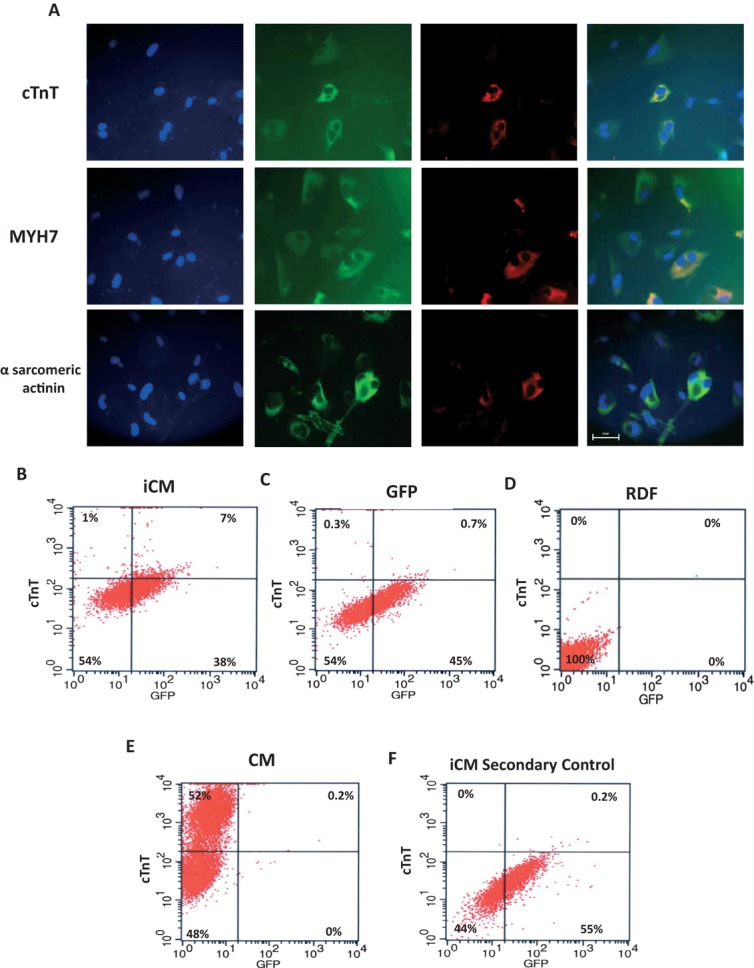
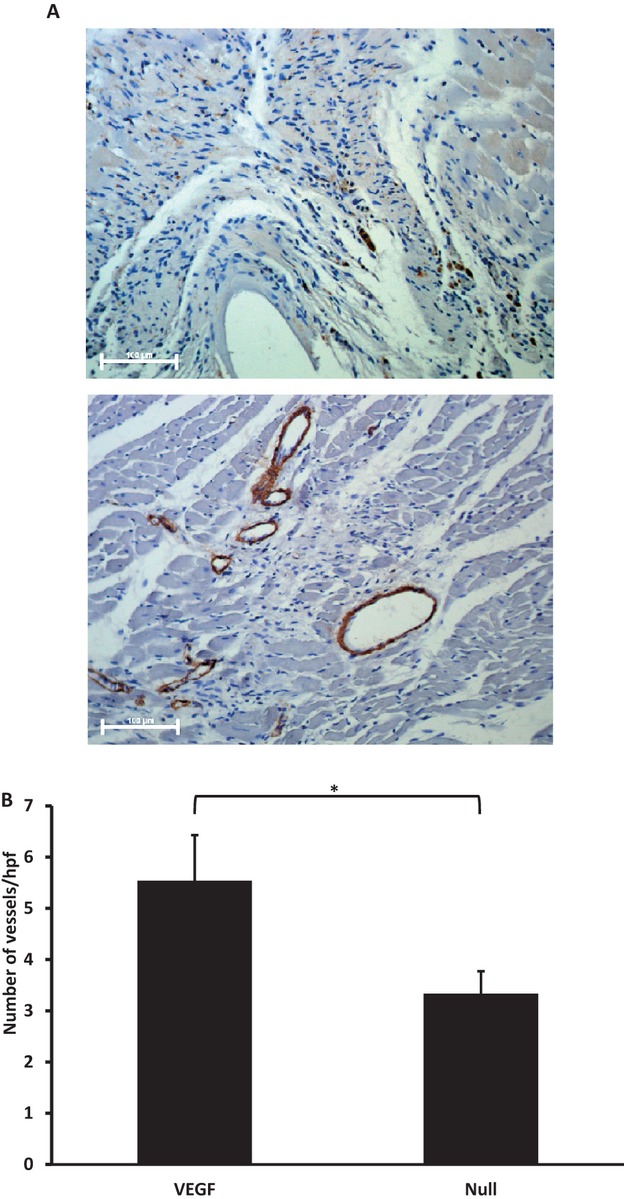
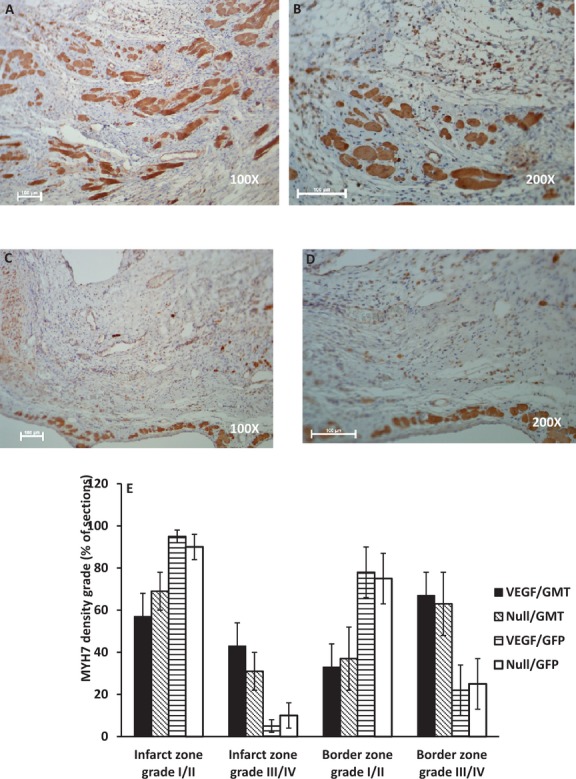
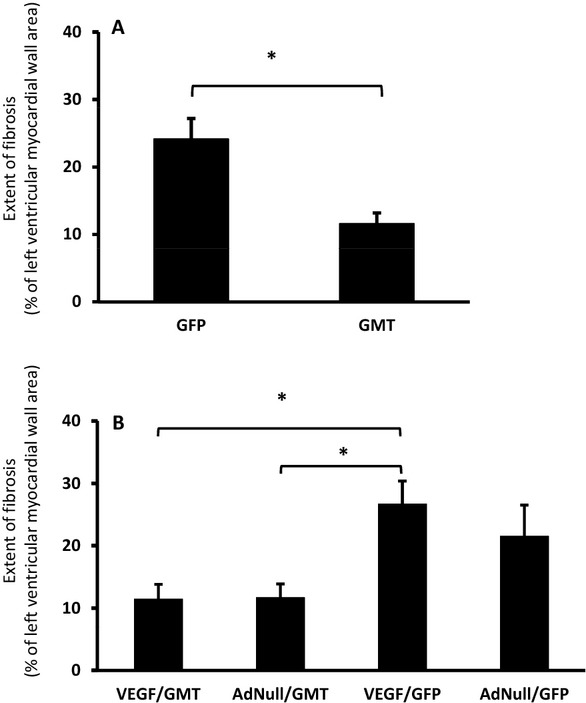
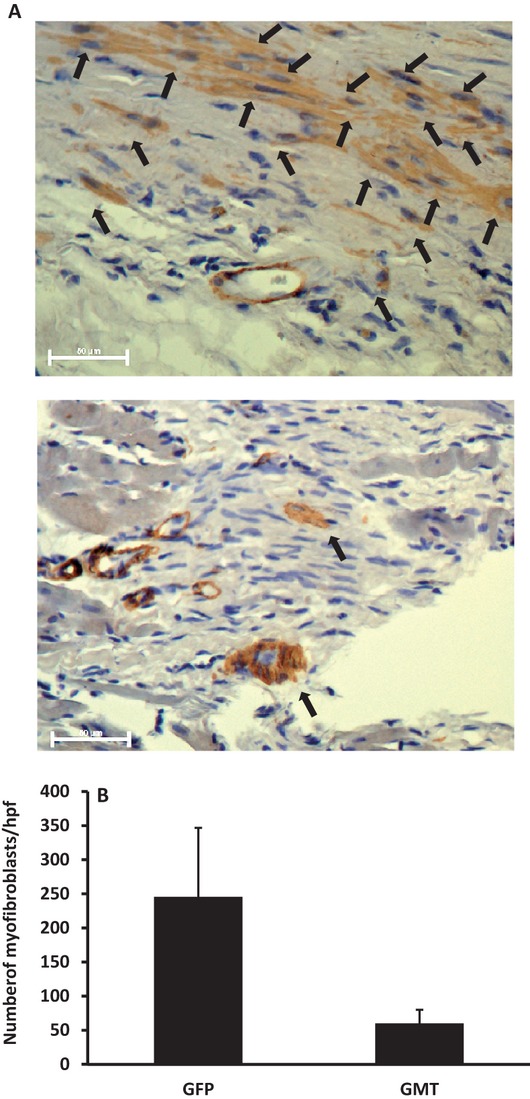
Gata4, Mef2c, and Tbx5 (GMT) administration via lentiviral transduction was demonstrated to transdifferentiate rat fibroblasts into (induced) cardiomyocytes in vitro by cardiomyocyte marker studies. Fisher 344 rats underwent coronary ligation and intramyocardial administration of an adenovirus encoding all 3 major isoforms of VEGF (AdVEGF-All6A(+)) or an AdNull control vector (n=12/group). Lentivirus encoding GMT or a GFP control was administered to each animal 3 weeks later, followed by histologic and echocardiographic analyses. GMT administration reduced the extent of fibrosis by half compared with GFP controls (12 ± 2% vs 24 ± 3%, P<0.01) and reduced the number of myofibroblasts detected in the infarct zone by 4-fold. GMT-treated animals also demonstrated greater density of cardiomyocyte-specific marker beta myosin heavy chain 7(+) cells compared with animals receiving GFP with or without VEGF (P<0.01). Ejection fraction was significantly improved after GMT vs GFP administration (12 ± 3% vs -7 ± 3%, P<0.01). Eight (73%) GFP animals but no GMT animals demonstrated decreased ejection fraction during this interval (P<0.01). Also, improvement in ejection fraction was 4-fold greater in GMT/VEGF vs GMT/null animals (17 ± 2% vs 4 ± 1%, P<0.05).
VEGF administration to infarcted myocardium enhances the efficacy of GMT-mediated cellular reprogramming in improving myocardial function and reducing the extent of myocardial fibrosis compared with the use of GMT or VEGF alone.
原位细胞重编程提供了一种可能性,可以直接从瘢痕成纤维细胞中再生功能性心肌细胞,从而避免细胞移植的挑战。我们假设,通过基因转导预先处理瘢痕组织,将血管生成的血管内皮生长因子(VEGF)转染到其中,将增强这种策略的疗效。
通过心肌细胞标志物研究,证明 Gata4、Mef2c 和 Tbx5(GMT)的慢病毒转导可将大鼠成纤维细胞体外转化为(诱导的)心肌细胞。Fisher 344 大鼠接受冠状动脉结扎和心肌内注射编码所有 3 种主要同工型 VEGF 的腺病毒(AdVEGF-All6A(+))或 AdNull 对照载体(每组 n=12)。3 周后,每只动物给予编码 GMT 或 GFP 对照的慢病毒,然后进行组织学和超声心动图分析。与 GFP 对照相比,GMT 给药使纤维化程度减半(12 ± 2%对 24 ± 3%,P<0.01),梗死区肌成纤维细胞数量减少 4 倍。GMT 治疗动物的心肌细胞特异性标志物β肌球蛋白重链 7(+)细胞密度也明显高于接受 GFP 治疗的动物,无论是否给予 VEGF(P<0.01)。与 GFP 给药相比,GMT 给药后射血分数显著改善(12 ± 3%对-7 ± 3%,P<0.01)。在这段时间内,8 只(73%)GFP 动物但没有 GMT 动物的射血分数下降(P<0.01)。此外,GMT/VEGF 组比 GMT/null 组射血分数改善幅度大 4 倍(17 ± 2%对 4 ± 1%,P<0.05)。
与单独使用 GMT 或 VEGF 相比,在梗死心肌中给予 VEGF 可增强 GMT 介导的细胞重编程改善心肌功能和减少心肌纤维化程度的疗效。