Department of Radiation Oncology, University of Utah, Salt Lake City, UT 84112, USA.
J Appl Clin Med Phys. 2013 Jan 7;14(1):4012. doi: 10.1120/jacmp.v14i1.4012.
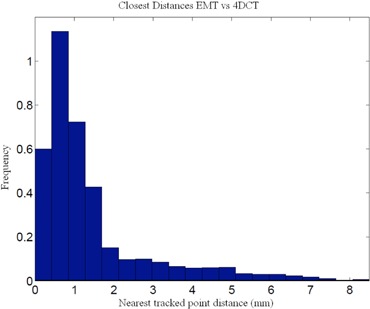
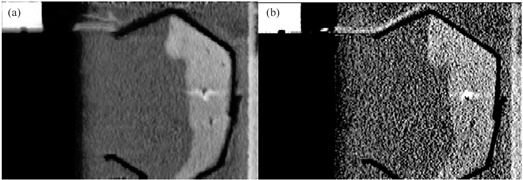
Calculation of four-dimensional (4D) dose distributions requires the remapping of dose calculated on each available binned phase of the 4D CT onto a reference phase for summation. Deformable image registration (DIR) is usually used for this task, but unfortunately almost always considers only endpoints rather than the whole motion path. A new algorithm, 4D tissue deformation reconstruction (4D TDR), that uses either CT projection data or all available 4D CT images to reconstruct 4D motion data, was developed. The purpose of this work is to verify the accuracy of the fit of this new algorithm using a realistic tissue phantom. A previously described fresh tissue phantom with implanted electromagnetic tracking (EMT) fiducials was used for this experiment. The phantom was animated using a sinusoidal and a real patient-breathing signal. Four-dimensional computer tomography (4D CT) and EMT tracking were performed. Deformation reconstruction was conducted using the 4D TDR and a modified 4D TDR which takes real tissue hysteresis (4D TDR(Hysteresis)) into account. Deformation estimation results were compared to the EMT and 4D CT coordinate measurements. To eliminate the possibility of the high contrast markers driving the 4D TDR, a comparison was made using the original 4D CT data and data in which the fiducials were electronically masked. For the sinusoidal animation, the average deviation of the 4D TDR compared to the manually determined coordinates from 4D CT data was 1.9 mm, albeit with as large as 4.5 mm deviation. The 4D TDR calculation traces matched 95% of the EMT trace within 2.8 mm. The motion hysteresis generated by real tissue is not properly projected other than at endpoints of motion. Sinusoidal animation resulted in 95% of EMT measured locations to be within less than 1.2 mm of the measured 4D CT motion path, enabling accurate motion characterization of the tissue hysteresis. The 4D TDR(Hysteresis) calculation traces accounted well for the hysteresis and matched 95% of the EMT trace within 1.6 mm. An irregular (in amplitude and frequency) recorded patient trace applied to the same tissue resulted in 95% of the EMT trace points within less than 4.5 mm when compared to both the 4D CT and 4D TDR(Hysteresis) motion paths. The average deviation of 4D TDR(Hysteresis) compared to 4D CT datasets was 0.9 mm under regular sinusoidal and 1.0 mm under irregular patient trace animation. The EMT trace data fit to the 4D TDR(Hysteresis) was within 1.6 mm for sinusoidal and 4.5 mm for patient trace animation. While various algorithms have been validated for end-to-end accuracy, one can only be fully confident in the performance of a predictive algorithm if one looks at data along the full motion path. The 4D TDR, calculating the whole motion path rather than only phase- or endpoints, allows us to fully characterize the accuracy of a predictive algorithm, minimizing assumptions. This algorithm went one step further by allowing for the inclusion of tissue hysteresis effects, a real-world effect that is neglected when endpoint-only validation is performed. Our results show that the 4D TDR(Hysteresis) correctly models the deformation at the endpoints and any intermediate points along the motion path.
计算四维(4D)剂量分布需要将 4D CT 上每个可用的-bin 相位的计算剂量映射到参考相位进行求和。通常使用变形图像配准(DIR)来完成此任务,但不幸的是,它几乎总是只考虑终点,而不是整个运动路径。开发了一种新的算法,即四维组织变形重建(4D TDR),该算法使用 CT 投影数据或所有可用的 4D CT 图像来重建 4D 运动数据。这项工作的目的是使用逼真的组织体模验证该新算法的拟合准确性。之前已经描述了一种具有植入电磁跟踪(EMT)基准的新鲜组织体模,用于进行此项实验。使用正弦和真实患者呼吸信号对体模进行动画处理。进行了四维计算机断层扫描(4D CT)和 EMT 跟踪。使用 4D TDR 和考虑实际组织滞后(4D TDR(滞后))的修改后的 4D TDR 进行变形重建。将变形估计结果与 EMT 和 4D CT 坐标测量值进行比较。为了消除高对比度标记驱动 4D TDR 的可能性,对原始 4D CT 数据和对基准进行电子屏蔽的数据进行了比较。对于正弦动画,4D TDR 与手动确定的 4D CT 数据坐标之间的平均偏差为 1.9 毫米,尽管最大偏差为 4.5 毫米。4D TDR 计算轨迹在 2.8 毫米内与 EMT 轨迹的 95%匹配。除了运动的端点之外,实际组织产生的运动滞后不能正确地投影。正弦动画导致 EMT 测量位置的 95%都在测量的 4D CT 运动路径的 1.2 毫米以内,从而能够准确地描述组织滞后的运动特征。4D TDR(滞后)计算轨迹很好地解释了滞后现象,并且在 1.6 毫米内与 EMT 轨迹的 95%匹配。将相同组织上记录的不规则(幅度和频率)患者轨迹应用于 4D TDR(滞后),与 4D CT 和 4D TDR(滞后)运动路径相比,95%的 EMT 轨迹点都在 4.5 毫米以内。在规则的正弦和不规则的患者轨迹动画下,4D TDR(滞后)与 4D CT 数据集之间的平均偏差分别为 0.9 毫米和 1.0 毫米。 EMT 轨迹数据与 4D TDR(滞后)的拟合度在正弦曲线为 1.6 毫米,在患者轨迹动画下为 4.5 毫米。虽然已经验证了各种算法的端到端准确性,但只有当沿着整个运动路径查看数据时,才能对预测算法的性能充满信心。4D TDR 计算整个运动路径,而不仅仅是相位或端点,使我们能够充分描述预测算法的准确性,从而最小化假设。该算法更进一步,允许包括组织滞后效应,这是在仅进行端点验证时被忽略的实际效应。我们的结果表明,4D TDR(滞后)正确地模拟了端点处的变形以及运动路径上的任何中间点。