Divisions of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, New York Medical College, Valhalla, NY, USA.
Arch Med Sci. 2012 Dec 20;8(6):957-69. doi: 10.5114/aoms.2012.32402. Epub 2012 Dec 19.
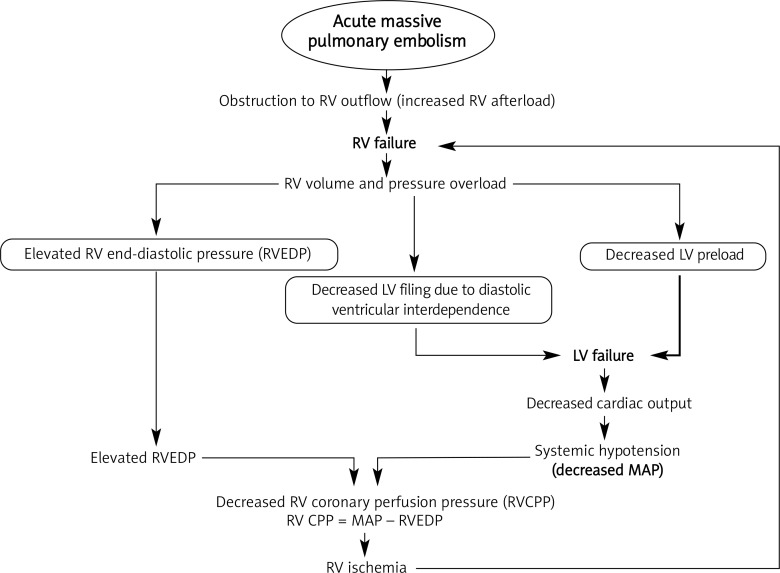
Massive pulmonary embolism (PE) is characterized by systemic hypotension (defined as a systolic arterial pressure < 90 mm Hg or a drop in systolic arterial pressure of at least 40 mm Hg for at least 15 min which is not caused by new onset arrhythmias) or shock (manifested by evidence of tissue hypoperfusion and hypoxia, including an altered level of consciousness, oliguria, or cool, clammy extremities). Massive pulmonary embolism has a high mortality rate despite advances in diagnosis and therapy. A subgroup of patients with nonmassive PE who are hemodynamically stable but with right ventricular (RV) dysfunction or hypokinesis confirmed by echocardiography is classified as submassive PE. Their prognosis is different from that of others with non-massive PE and normal RV function. This article attempts to review the evidence-based risk stratification, diagnosis, initial stabilization, and management of massive and nonmassive pulmonary embolism.
大面积肺栓塞(PE)的特征是全身性低血压(定义为收缩压<90mmHg 或收缩压至少下降 40mmHg 持续至少 15min,且不是由新发心律失常引起的)或休克(表现为组织灌注和缺氧的证据,包括意识改变、少尿或四肢发凉、发绀)。尽管在诊断和治疗方面取得了进展,但大面积肺栓塞的死亡率仍然很高。一小部分非大面积 PE 患者血流动力学稳定,但超声心动图证实右心室(RV)功能障碍或运动不良,被归类为亚大面积 PE。他们的预后与其他非大面积 PE 且 RV 功能正常的患者不同。本文试图回顾大面积和非大面积肺栓塞的基于循证的风险分层、诊断、初步稳定和管理。