Aganovic Damir, Prcic Alden, Hadziosmanovic Osman, Hasanbegovic Munira
Department of Urology, Clinical Centre of University of Sarajevo, Bosnia and Herzegovina.
Acta Inform Med. 2012 Sep;20(3):160-6. doi: 10.5455/aim.2012.20.160-166.
Determine diagnostic power and intercorrelation between bladder outlet obstruction number (BOON) and intravesical prostatic protrusion (IPP ) as non-invasive predictors of infravesical obstruction in patients with lower urinary tract symptoms due to benign prostatic enlargement.
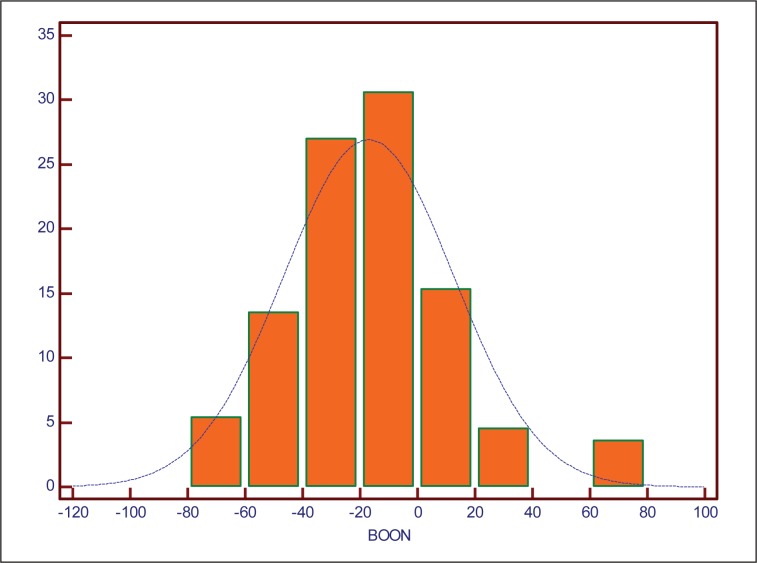
Prospective study during 2009-2010 analyzed data of 110 patients with proven benign prostatic enlargement. Prostate volume and IPP were determined by transabdominal ultrasound, and patients underwent complete urodynamic studies (UDS). BOON was calculated using the formula: prostate volume (cc)-3 x Qmax (ml/s)-0.2 x mean voided volume (ml).
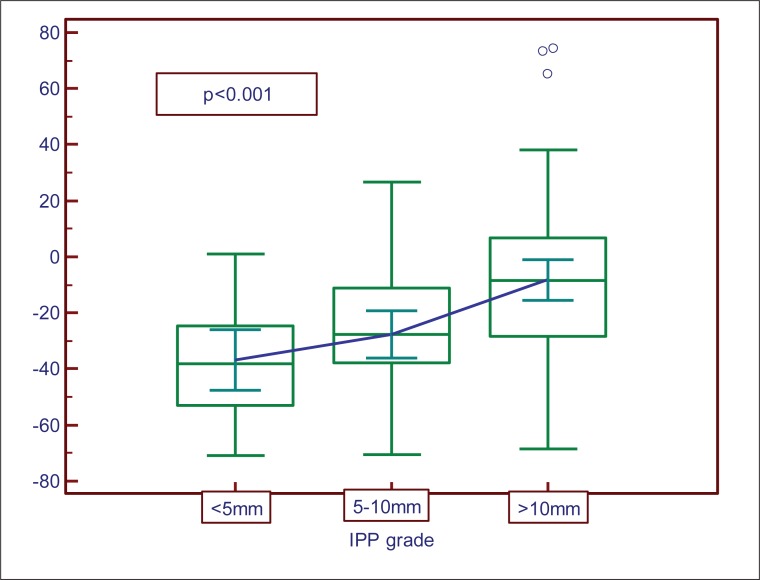
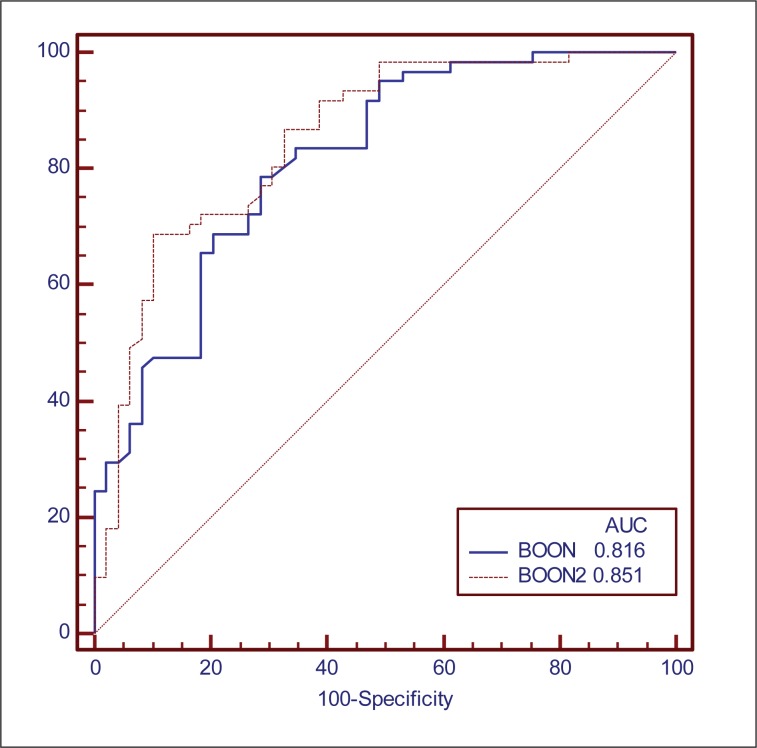
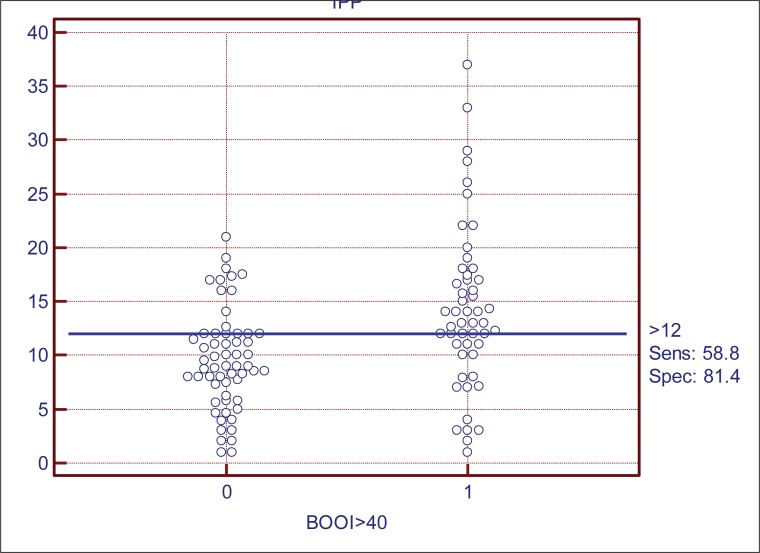
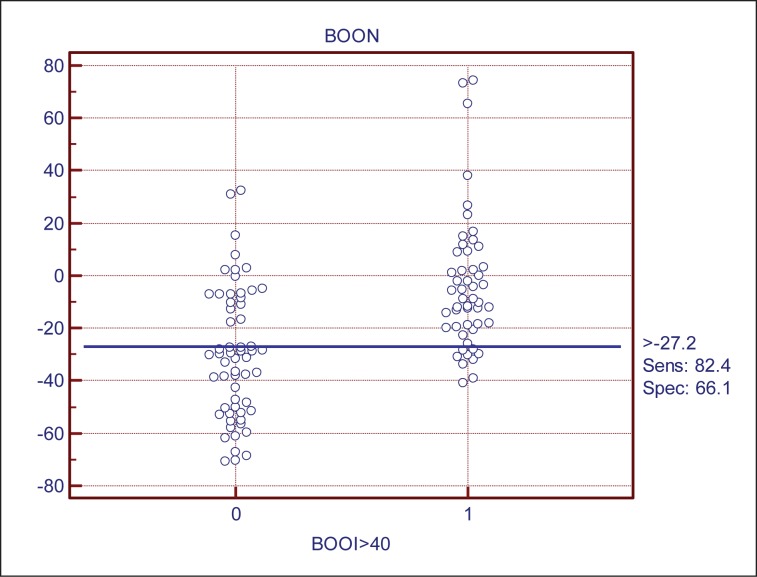
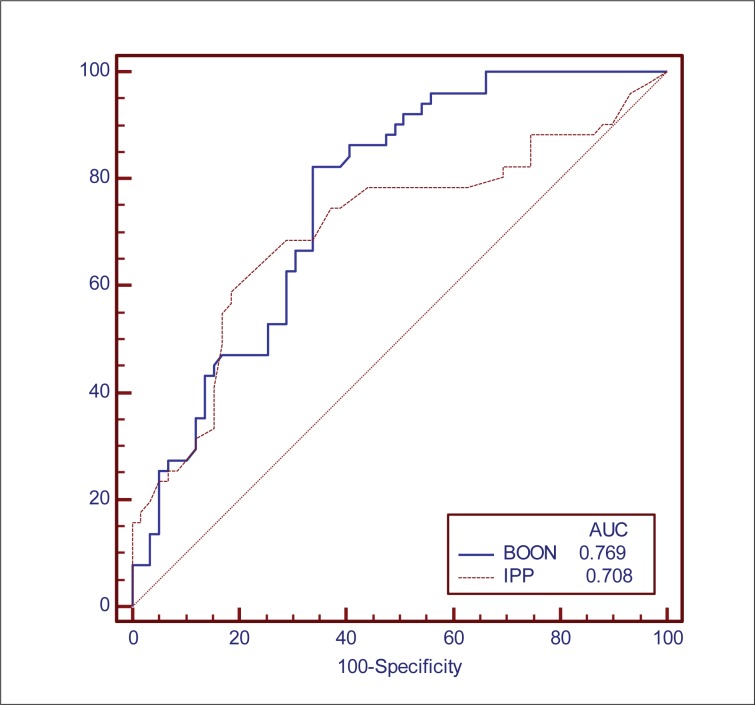
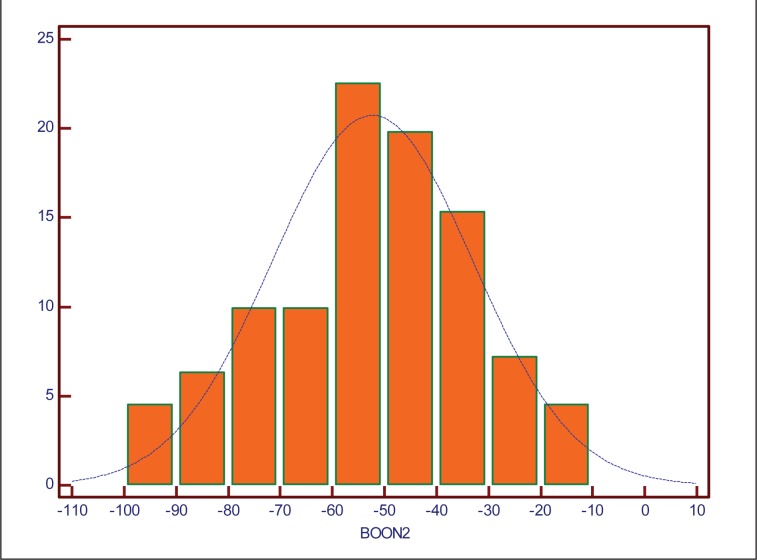
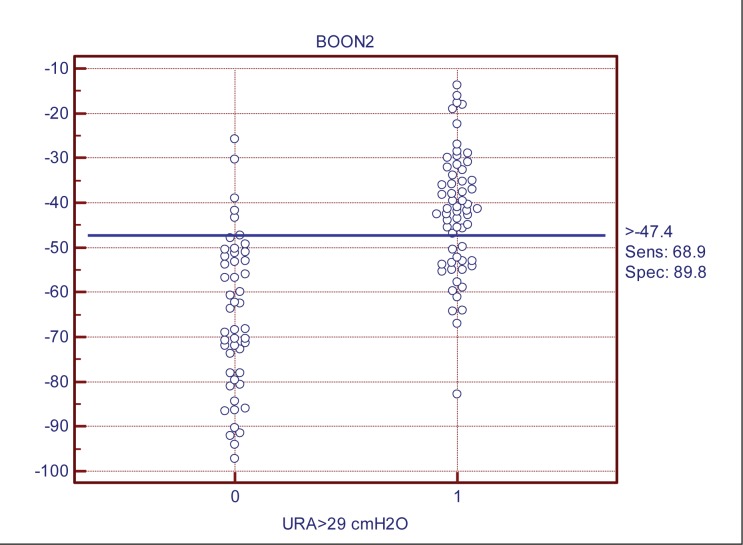
There is a statistically significant correlation between the values of IPP and BOON (Spearman's rank correlation coefficient rho=0.48, p=0.0001). BOON is a more sensitive (sensitivity 82.4%, specificity 66.1%), while IPP is a more specific factor (sensitivity 58.8%, specificity 81.4%) in the group-wise prediction of bladder outlet obstruction (BOO). Positive predictive value in the diagnosis of obstruction increases at the individual level combining the cut-off values for BOON>-30, with IPP >10 mm (PP V 86.8%). Owing to a good correlation of IPP with different definitions of urodynamic obstruction, IPP was included in the BOON formula instead of prostate volume. This number was arbitrarily called BOON2. The combination of IPP >10 mm and cut-off value for BOON2 >-50 showed that 88.6% of the patients were accurately classified in the zone of obstruction (mean IPP 14.9 mm), while BOON2<-50 carried a high NPV.
The combination of cut-off values for BOON and IPP increases test accuracy according to BOO at the individual level, thus facilitating clinical decision making regarding diagnostics and optimal choice of therapy in patients with BPE. Owing to its good correlation with obstruction determinants, IPP can be included in the formula for BOON instead of prostate volume.
确定膀胱出口梗阻指数(BOON)和膀胱内前列腺突入(IPP)作为良性前列腺增生所致下尿路症状患者膀胱以下梗阻的非侵入性预测指标的诊断效能及相互关系。
2009年至2010年进行的前瞻性研究分析了110例经证实为良性前列腺增生患者的数据。经腹部超声测定前列腺体积和IPP,患者接受完整的尿动力学检查(UDS)。BOON使用公式计算:前列腺体积(立方厘米)-3×最大尿流率(毫升/秒)-0.2×平均排尿量(毫升)。
IPP和BOON值之间存在统计学显著相关性(斯皮尔曼等级相关系数rho = 0.48,p = 0.0001)。在分组预测膀胱出口梗阻(BOO)方面,BOON更敏感(敏感性82.4%,特异性66.1%),而IPP是更具特异性的因素(敏感性58.8%,特异性81.4%)。在个体水平上,将BOON > -30与IPP > 10毫米的临界值相结合,梗阻诊断的阳性预测值增加(PP V 86.8%)。由于IPP与尿动力学梗阻的不同定义具有良好的相关性,因此在BOON公式中用IPP代替了前列腺体积。这个数值被随意称为BOON2。IPP > 10毫米与BOON2 > -50的临界值相结合显示,88.6%的患者被准确分类到梗阻区域(平均IPP为