Department of Radiation Oncology, The Catholic University of Korea, College of Medicine, Seoul, South Korea.
Radiat Oncol. 2013 Jan 16;8:15. doi: 10.1186/1748-717X-8-15.
We want to evaluate the efficacy of helical tomotherapy (HT) for treating advanced hepatocellular carcinoma (HCC) with portal vein tumor thrombosis (PVTT).
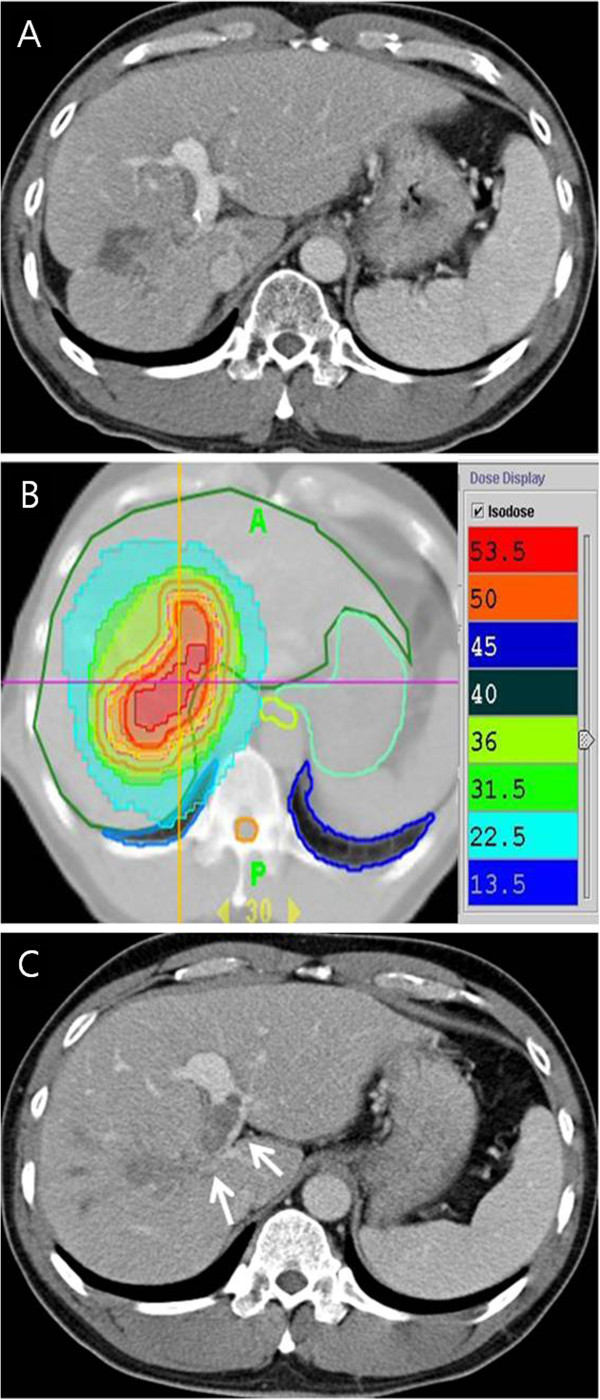
We treated 35 patients for unresectable HCC combined with PVTT in whom other treatment modalities were not indicated. The tumor thrombi involved the main trunk of the portal vein in 18 patients (51.4%) and the first or second order branches in 17 patients (48.6%). A median dose of 50 Gy (range: 45-60 Gy) was delivered in 10 fractions. Capecitabine was given concomitantly at a dose of 600 mg/m2 twice daily during radiotherapy.
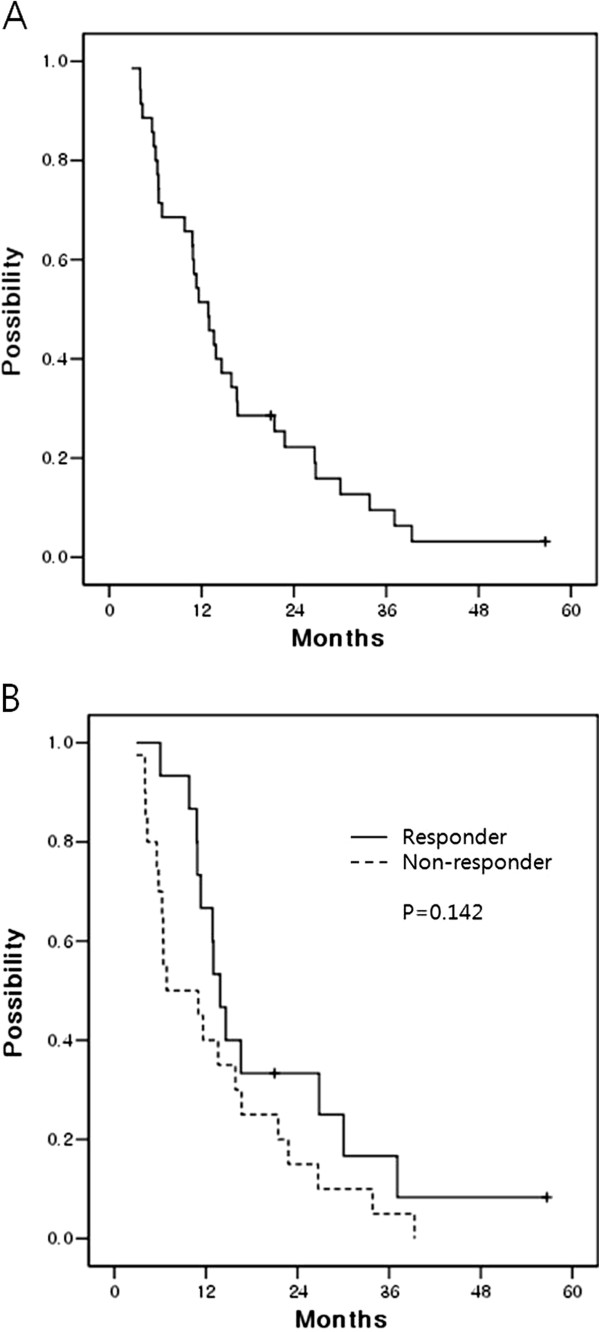
The responses were evaluated via computed tomography. There was a complete response (CR) in 5 patients (14.3%), partial response (PR) in 10 patients (28.6%), stable disease (SD) in 18 patients (51.4%) and progressive disease (PD) in 2 patients (5.7%). The Child-Pugh classification (A vs B) and the Japan integrated staging (JIS) score (2 vs 3) were statistically significant parameters that predicted the response of PVTT (p = 0.010 and p = 0.026, respectively). The median survival, one and two year survival rate of all patients was 12.9 months, 51.4% and 22.2%, respectively. The patients with tumor thrombi in the main portal trunk showed statistically inferior overall survival than patients with tumor thrombi in the portal vein branches (9.8 versus 16.6 months, respectively, p = 0.036). The responders' median survival was 13.9 months, double 6.9 months as the median survival of the non-responders. No radiation induced liver disease or treatment related mortality was not appeared.
Hypofractionated radiotherapy with HT was effective not only for tumor response but also for survival in the advanced HCC patients with PVTT. And stricter patient selection by Child-Pugh classification and JIS score may maximize the potential benefits of this treatment.
我们旨在评估螺旋断层放疗(HT)治疗合并门静脉癌栓(PVTT)的不可切除肝细胞癌(HCC)的疗效。
我们对 35 例不适合其他治疗方法的不可切除 HCC 合并 PVTT 患者进行了治疗。18 例(51.4%)患者门静脉主干癌栓,17 例(48.6%)患者第一或第二级分支癌栓。中位剂量为 50 Gy(范围:45-60 Gy),分 10 次给予。放疗期间同时给予卡培他滨,剂量为 600 mg/m2,每日 2 次。
通过计算机断层扫描评估反应。5 例(14.3%)患者完全缓解(CR),10 例(28.6%)患者部分缓解(PR),18 例(51.4%)患者疾病稳定(SD),2 例(5.7%)患者疾病进展(PD)。Child-Pugh 分级(A 级与 B 级)和日本综合分期(JIS)评分(2 级与 3 级)是预测 PVTT 反应的统计学显著参数(p=0.010 和 p=0.026)。所有患者的中位生存时间、1 年和 2 年生存率分别为 12.9 个月、51.4%和 22.2%。主门静脉主干癌栓患者的总生存明显劣于门静脉分支癌栓患者(9.8 个月比 16.6 个月,p=0.036)。有反应者的中位生存时间为 13.9 个月,是无反应者的 6.9 个月的两倍。未出现放射性肝损伤或治疗相关死亡。
对于合并 PVTT 的晚期 HCC 患者,HT 低分割放疗不仅对肿瘤反应有效,而且对生存也有效。通过 Child-Pugh 分级和 JIS 评分进行更严格的患者选择,可能最大限度地发挥这种治疗的潜在益处。