General Internal Medicine and Infectious Diseases, Ghent University Hospital, Ghent, Belgium.
PLoS One. 2013;8(1):e52562. doi: 10.1371/journal.pone.0052562. Epub 2013 Jan 9.
Optimal regimen choice of antiretroviral therapy is essential to achieve long-term clinical success. Integrase inhibitors have swiftly been adopted as part of current antiretroviral regimens. The purpose of this study was to review the evidence for integrase inhibitor use in clinical settings.
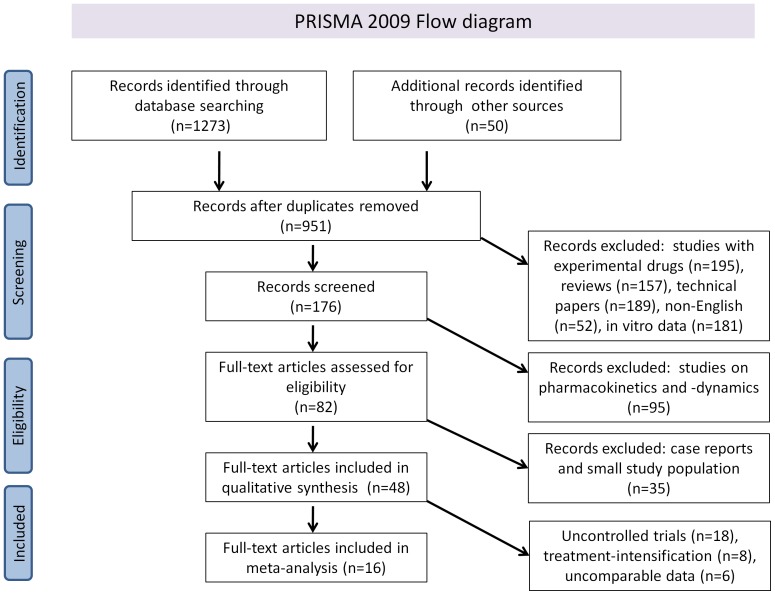
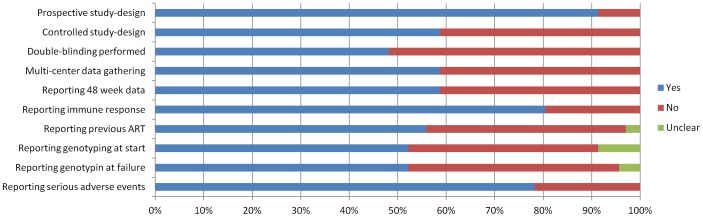
MEDLINE and Web-of-Science were screened from April 2006 until November 2012, as were hand-searched scientific meeting proceedings. Multiple reviewers independently screened 1323 citations in duplicate to identify randomized controlled trials, nonrandomized controlled trials and cohort studies on integrase inhibitor use in clinical practice. Independent, duplicate data extraction and quality assessment were conducted.
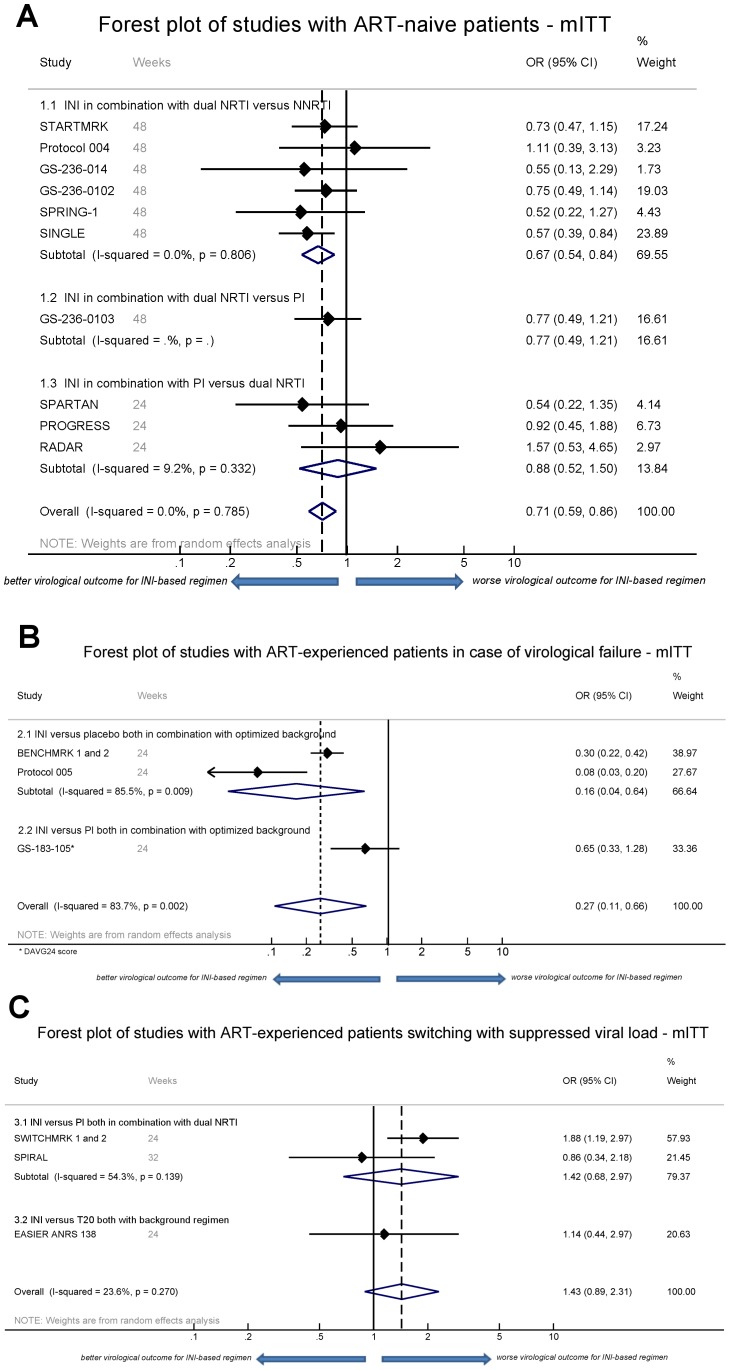
48 unique studies were included on the use of integrase inhibitors in antiretroviral therapy-naive patients and treatment-experienced patients with either virological failure or switching to integrase inhibitors while virologically suppressed. On the selected studies with comparable outcome measures and indication (n = 16), a meta-analysis was performed based on modified intention-to-treat (mITT), on-treatment (OT) and as-treated (AT) virological outcome data. In therapy-naive patients, favorable odds ratios (OR) for integrase inhibitor-based regimens were observed, (mITT OR 0.71, 95% CI 0.59-0.86). However, integrase inhibitors combined with protease inhibitors only did not result in a significant better virological outcome. Evidence further supported integrase inhibitor use following virological failure (mITT OR 0.27; 95% CI 0.11-0.66), but switching to integrase inhibitors from a high genetic barrier drug during successful treatment was not supported (mITT OR 1.43; 95% CI 0.89-2.31). Integrase inhibitor-based regimens result in similar immunological responses compared to other regimens. A low genetic barrier to drug-resistance development was observed for raltegravir and elvitegravir, but not for dolutegravir.
In first-line therapy, integrase inhibitors are superior to other regimens. Integrase inhibitor use after virological failure is supported as well by the meta-analysis. Careful use is however warranted when replacing a high genetic barrier drug in treatment-experienced patients switching successful treatment.
选择最佳的抗逆转录病毒治疗方案对于实现长期临床成功至关重要。整合酶抑制剂已迅速成为当前抗逆转录病毒治疗方案的一部分。本研究旨在综述整合酶抑制剂在临床应用中的证据。
从 2006 年 4 月至 2012 年 11 月,我们对 MEDLINE 和 Web-of-Science 进行了筛选,并对科学会议论文集进行了手工检索。多名评审员独立对 1323 条引文进行了重复筛选,以确定整合酶抑制剂在临床实践中用于初治患者和治疗失败或在病毒学抑制时转换为整合酶抑制剂的治疗经验患者的随机对照试验、非随机对照试验和队列研究。进行了独立的、重复的数据提取和质量评估。
共有 48 项关于初治患者和治疗失败或转换为整合酶抑制剂时病毒学抑制患者使用整合酶抑制剂的研究被纳入,纳入的研究具有可比性的结局指标和适应证(n=16),我们基于改良意向治疗(mITT)、治疗期间(OT)和实际治疗(AT)的病毒学结局数据进行了荟萃分析。在初治患者中,观察到基于整合酶抑制剂的方案具有有利的优势比(OR),(mITT OR 0.71,95%CI 0.59-0.86)。然而,整合酶抑制剂与蛋白酶抑制剂联合应用并未导致病毒学结局的显著改善。证据进一步支持整合酶抑制剂在病毒学失败后使用(mITT OR 0.27;95%CI 0.11-0.66),但在成功治疗时从高遗传屏障药物转换为整合酶抑制剂并不支持(mITT OR 1.43;95%CI 0.89-2.31)。与其他方案相比,整合酶抑制剂方案的免疫反应相似。拉替拉韦和艾维雷韦耐药的遗传屏障较低,但多替拉韦则不然。
在一线治疗中,整合酶抑制剂优于其他方案。荟萃分析也支持病毒学失败后使用整合酶抑制剂。然而,在治疗经验患者转换成功治疗时,需要谨慎使用替换高遗传屏障药物。