Lord Katherine, De León Diva D
Division of Endocrinology and Diabetes, The Children's Hospital of Philadelphia, 3615 Civic Center Boulevard, Abramson Research Center Room 802A, Philadelphia, PA, 19104, USA.
Int J Pediatr Endocrinol. 2013 Feb 6;2013(1):3. doi: 10.1186/1687-9856-2013-3.
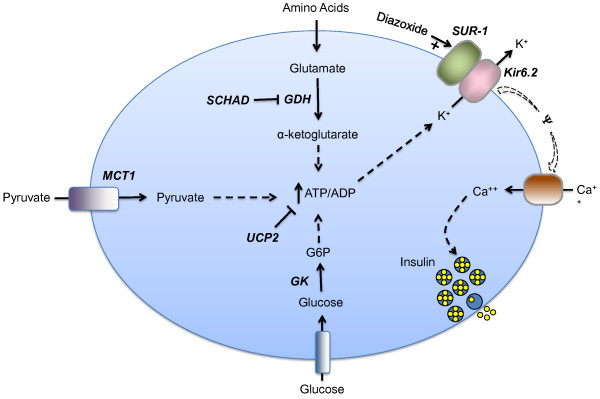
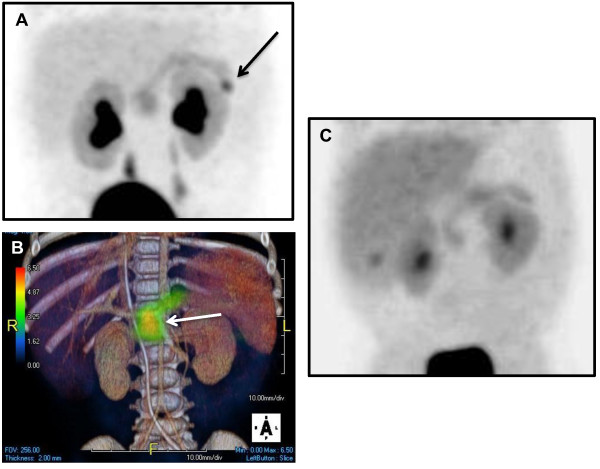
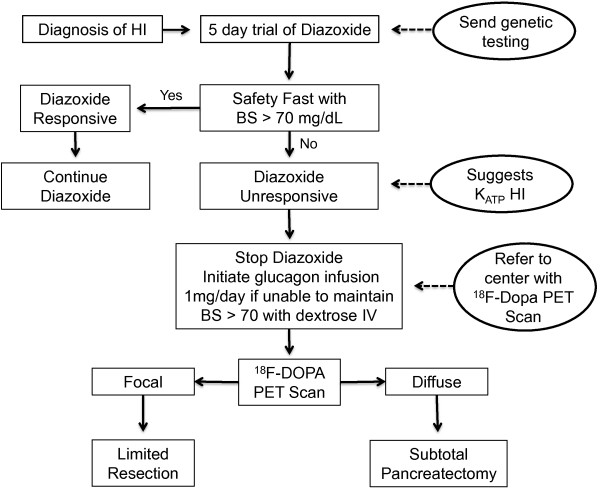
Hyperinsulinism (HI) is the leading cause of persistent hypoglycemia in children, which if unrecognized may lead to development delays and permanent neurologic damage. Prompt recognition and appropriate treatment of HI are essential to avoid these sequelae. Major advances have been made over the past two decades in understanding the molecular basis of hyperinsulinism and mutations in nine genes are currently known to cause HI. Inactivating KATP channel mutations cause the most common and severe type of HI, which occurs in both a focal and a diffuse form. Activating mutations of glutamate dehydrogenase (GDH) lead to hyperinsulinism/hyperammonemia syndrome, while activating mutations of glucokinase (GK), the "glucose sensor" of the beta cell, causes hyperinsulinism with a variable clinical phenotype. More recently identified genetic causes include mutations in the genes encoding short-chain 3-hydroxyacyl-CoA (SCHAD), uncoupling protein 2 (UCP2), hepatocyte nuclear factor 4-alpha (HNF-4α), hepatocyte nuclear factor 1-alpha (HNF-1α), and monocarboyxlate transporter 1 (MCT-1), which results in a very rare form of HI triggered by exercise. For a timely diagnosis, a critical sample and a glucagon stimulation test should be done when plasma glucose is < 50 mg/dL. A failure to respond to a trial of diazoxide, a KATP channel agonist, suggests a KATP defect, which frequently requires pancreatectomy. Surgery is palliative for children with diffuse KATPHI, but children with focal KATPHI are cured with a limited pancreatectomy. Therefore, distinguishing between diffuse and focal disease and localizing the focal lesion in the pancreas are crucial aspects of HI management. Since 2003, 18 F-DOPA PET scans have been used to differentiate diffuse and focal disease and localize focal lesions with higher sensitivity and specificity than more invasive interventional radiology techniques. Hyperinsulinism remains a challenging disorder, but recent advances in the understanding of its genetic basis and breakthroughs in management should lead to improved outcomes for these children.
高胰岛素血症(HI)是儿童持续性低血糖的主要原因,若未被识别,可能导致发育迟缓及永久性神经损伤。及时识别并恰当治疗HI对于避免这些后遗症至关重要。在过去二十年里,在理解高胰岛素血症的分子基础方面取得了重大进展,目前已知九个基因的突变可导致HI。KATP通道失活突变会引发最常见且最严重的HI类型,其有局灶性和弥漫性两种形式。谷氨酸脱氢酶(GDH)的激活突变会导致高胰岛素血症/高氨血症综合征,而β细胞的“葡萄糖传感器”葡萄糖激酶(GK)的激活突变会导致具有可变临床表型的高胰岛素血症。最近发现的遗传病因包括编码短链3 - 羟基酰基辅酶A(SCHAD)、解偶联蛋白2(UCP2)、肝细胞核因子4α(HNF - 4α)、肝细胞核因子1α(HNF - 1α)和单羧酸转运蛋白1(MCT - 1)的基因突变,这些突变会导致一种由运动引发的非常罕见的HI形式。为了及时诊断,当血浆葡萄糖<50mg/dL时,应采集关键样本并进行胰高血糖素刺激试验。对KATP通道激动剂二氮嗪试验无反应提示存在KATP缺陷,这通常需要进行胰腺切除术。手术对弥漫性KATPHI患儿具有姑息作用,但局灶性KATPHI患儿通过有限的胰腺切除术可治愈。因此,区分弥漫性和局灶性疾病以及在胰腺中定位局灶性病变是HI管理的关键方面。自2003年以来,18F - DOPA PET扫描已被用于区分弥漫性和局灶性疾病,并以比侵入性更强的介入放射学技术更高的灵敏度和特异性来定位局灶性病变。高胰岛素血症仍然是一种具有挑战性的疾病,但最近在其遗传基础理解方面的进展以及管理上的突破应该会改善这些患儿的预后。