Centre for Tropical Diseases (CTD), Sacro Cuore Hospital, Negrar, Verona, Italy.
BMC Infect Dis. 2013 Feb 8;13:78. doi: 10.1186/1471-2334-13-78.
Strongyloidiasis is commonly a clinically unapparent, chronic infection, but immuno suppressed subjects can develop fatal disease. We carried out a review of literature on hyperinfection syndrome (HS) and disseminated strongyloidiasis (DS), in order to describe the most challenging aspects of severe strongyloidiasis.
We conducted a structured search using PubMed to collect case reports and short case series on HS/DS published from 1991 to 2011. We restricted search to papers in English, Spanish, Italian and French. Case reports were classified as HS/DS according to given definitions.
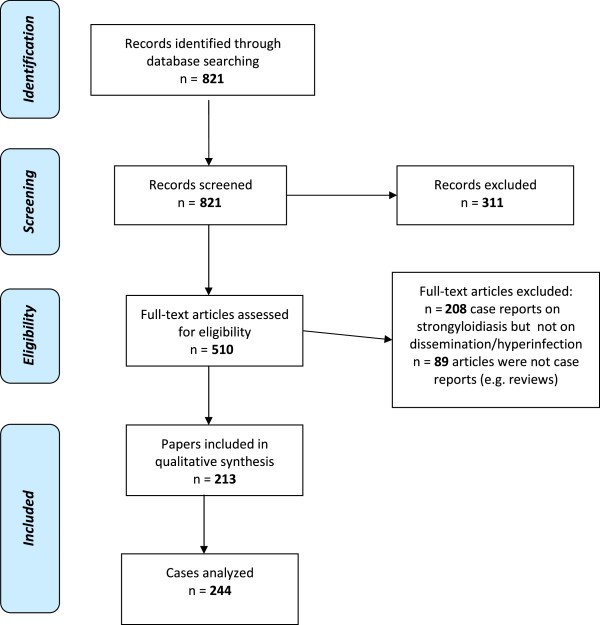
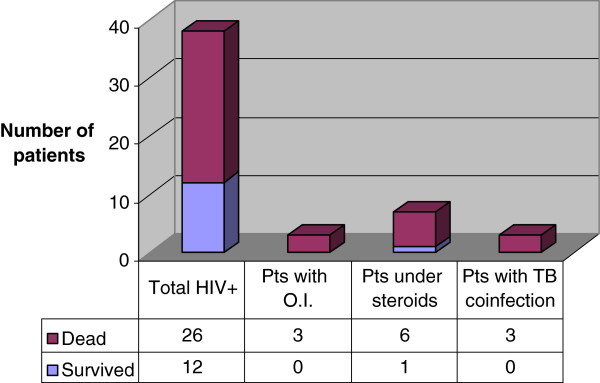
Records screened were 821, and 311 were excluded through titles and abstract evaluation. Of 510 full-text articles assessed for eligibility, 213 were included in qualitative analysis. As some of them were short case series, eventually the number of cases analyzed was 244.Steroids represented the main trigger predisposing to HS and DS (67% cases): they were mostly administered to treat underlying conditions (e.g. lymphomas, rheumatic diseases). However, sometimes steroids were empirically prescribed to treat signs and symptoms caused by unsuspected/unrecognized strongyloidiasis. Diagnosis was obtained by microscopy examination in 100% cases, while serology was done in a few cases (6.5%). Only in 3/29 cases of solid organ/bone marrow transplantation there is mention of pre-transplant serological screening. Therapeutic regimens were different in terms of drugs selection and combination, administration route and duration. Similar fatality rate was observed between patients with DS (68.5%) and HS (60%).
Proper screening (which must include serology) is mandatory in high - risk patients, for instance candidates to immunosuppressive medications, currently or previously living in endemic countries. In some cases, presumptive treatment might be justified. Ivermectin is the gold standard for treatment, although the optimal dosage is not clearly defined in case of HS/DS.
类圆线虫病通常是一种临床无症状的慢性感染,但免疫抑制的患者可能会发展为致命的疾病。我们对严重类圆线虫病的最具挑战性的方面进行了文献回顾,包括过感染综合征(HS)和播散性类圆线虫病(DS)。
我们使用 PubMed 进行了结构化搜索,以收集 1991 年至 2011 年期间发表的关于 HS/DS 的病例报告和短篇病例系列。我们将搜索范围限制在英文、西班牙文、意大利文和法文的论文。根据给出的定义,病例报告被归类为 HS/DS。
筛选出的记录为 821 条,通过标题和摘要评估排除了 311 条。在评估合格的 510 篇全文文章中,有 213 篇被纳入定性分析。由于其中一些是短篇病例系列,最终分析的病例数为 244 例。类固醇是导致 HS 和 DS 的主要诱因(67%的病例):它们主要用于治疗潜在疾病(如淋巴瘤、风湿性疾病)。然而,有时类固醇是为了治疗因未被怀疑/未被发现的类圆线虫病引起的症状和体征而经验性地开的。所有病例均通过显微镜检查获得诊断,而在少数情况下(6.5%)进行了血清学检查。仅在 29 例实体器官/骨髓移植中有 3 例提及移植前血清学筛查。治疗方案在药物选择和组合、给药途径和持续时间方面有所不同。DS(68.5%)和 HS(60%)患者的死亡率相似。
在高危患者中,必须进行适当的筛查(包括血清学检查),例如接受免疫抑制药物治疗的患者,目前或以前生活在流行地区的患者。在某些情况下,推定治疗可能是合理的。伊维菌素是治疗的金标准,尽管在 HS/DS 情况下,最佳剂量尚未明确。