Quigley Charmian A, Zagar Anthony J, Liu Charlie Chunhua, Brown David M, Huseman Carol, Levitsky Lynne, Repaske David R, Tsalikian Eva, Chipman John J
Lilly Research Laboratories, Indianapolis, IN 46285, USA.
Int J Pediatr Endocrinol. 2013 Feb 13;2013(1):6. doi: 10.1186/1687-9856-2013-6.
Many patients with childhood-onset growth hormone (GH) deficiency do not fulfill diagnostic criteria for GH deficiency (GHD) after attainment of adult height and may not require long-term GH treatment. Patients with history of idiopathic GHD (IGHD) pose the greatest management dilemma, as data regarding factors predictive of persistent GHD in this group are lacking.
The objective of this study was to assess potential predictors of persistent GHD in a US patient cohort during transition from childhood to adulthood, particularly in patients with history of IGHD.
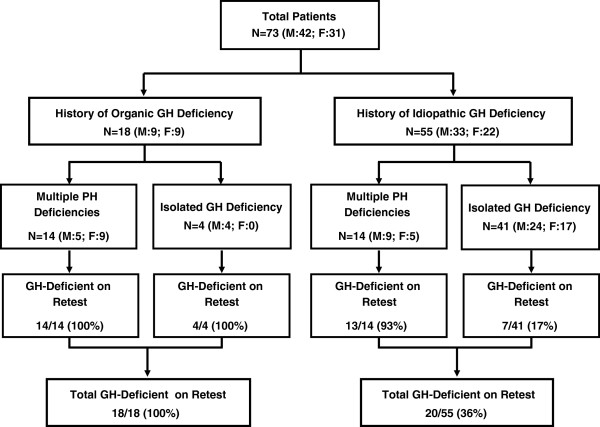
We studied 73 US patients with history of childhood-onset GHD screened at 21 US pediatric endocrine centers for a randomized clinical trial of GH replacement after attainment of adult height. The cohort comprised 42 boys/men and 31 girls/women aged14-22 years, who had received ≥1 year of GH treatment and had completed linear growth. The main outcome measures were sensitivity, specificity, positive and negative predictive values (PPV, NPV) of clinical and hormonal factors for persistent GHD (defined a priori in this study as peak GH < 5 μg/L).
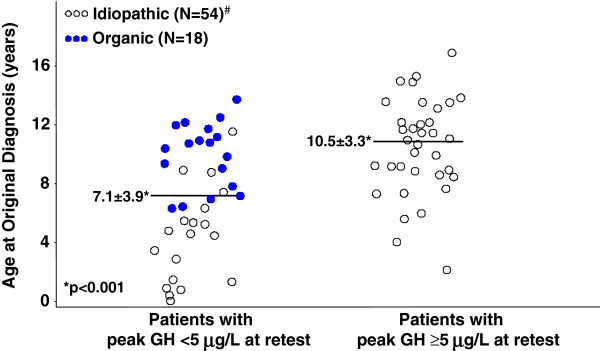
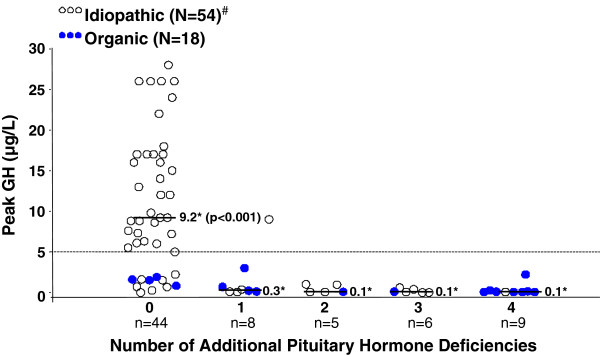
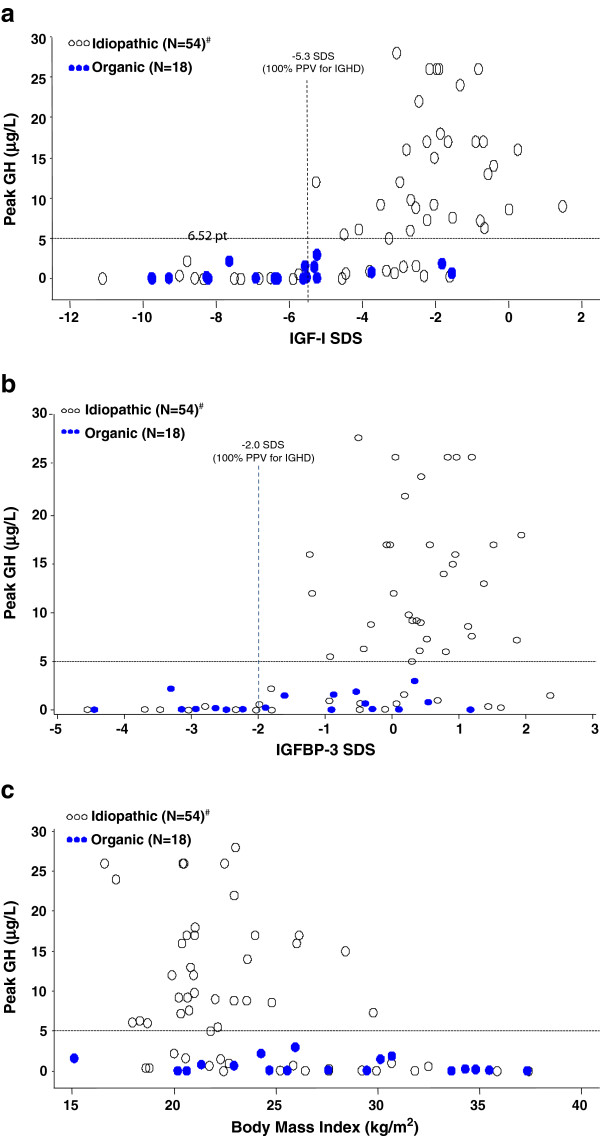
For the cohort as a whole, the best predictors of persistent GHD (100% PPV) were history of organic hypothalamic-pituitary disorder or ≥2 additional pituitary hormone deficiencies (PHD). Best predictors of persistent GHD in patients with childhood history of IGHD were standard deviation scores (SDS) for serum insulin-like growth factor binding protein-3 (IGFBP-3) below -2.0, and for insulin-like growth factor-I (IGF-I) below -5.3 (measured ≥6 weeks after completion of GH treatment; PPV 100% for both), and age <4 years at original diagnosis (PPV 89%). IGF-I above -1.6 SDS had 100% NPV.
US patients with an organic cause of childhood-onset GHD or ≥2 additional PHDs may not require GH stimulation testing to reconfirm GHD after completion of childhood treatment. In contrast, patients with idiopathic childhood-onset GHD almost invariably require retesting, as GHD persists in only a minority (those who were very young at initial diagnosis and those who have subnormal IGFBP-3 or extremely low IGF-I after completion of childhood treatment). Subnormal posttreatment IGF-I (<-2.0 SDS) lacked predictive power for persistent GHD, whereas IGF-I > -1.6 SDS was 100% predictive of GH sufficiency.
许多儿童期起病的生长激素(GH)缺乏症患者在达到成人身高后不符合GH缺乏症(GHD)的诊断标准,可能不需要长期GH治疗。特发性GHD(IGHD)病史的患者带来了最大的管理难题,因为缺乏该组中预测持续性GHD的因素的数据。
本研究的目的是评估美国一组患者从儿童期到成年期过渡期间持续性GHD的潜在预测因素,特别是有IGHD病史的患者。
我们研究了73名有儿童期起病GHD病史的美国患者,这些患者在美国21个儿科内分泌中心接受筛查,以进行一项关于成年身高后GH替代的随机临床试验。该队列包括42名男孩/男性和31名女孩/女性,年龄在14 - 22岁之间,他们接受了≥1年的GH治疗且已完成线性生长。主要结局指标是临床和激素因素对持续性GHD(本研究中预先定义为峰值GH < 5 μg/L)的敏感性、特异性、阳性和阴性预测值(PPV、NPV)。
对于整个队列,持续性GHD的最佳预测因素(PPV为100%)是器质性下丘脑 - 垂体疾病史或≥2种其他垂体激素缺乏(PHD)。有儿童期IGHD病史患者持续性GHD的最佳预测因素是血清胰岛素样生长因子结合蛋白 - 3(IGFBP - 3)的标准差评分(SDS)低于 - 2.0,以及胰岛素样生长因子 - I(IGF - I)低于 - 5.3(在GH治疗完成后≥6周测量;两者的PPV均为100%),以及初诊时年龄<4岁(PPV为89%)。IGF - I高于 - 1.6 SDS的NPV为100%。
有儿童期起病GHD器质性病因或≥2种其他PHD的美国患者在儿童期治疗完成后可能不需要进行GH刺激试验来重新确认GHD。相比之下,有儿童期起病特发性GHD的患者几乎总是需要重新检测,因为只有少数患者(初诊时非常年幼以及儿童期治疗完成后IGFBP - 3低于正常或IGF - I极低的患者)存在持续性GHD。治疗后IGF - I低于正常(<-2.0 SDS)对持续性GHD缺乏预测能力,而IGF - I > - 1.6 SDS对GH充足性的预测率为100%。