Warwick Business School, Warwick University, Coventry, UK.
BMJ Open. 2013 Feb 20;3(2). doi: 10.1136/bmjopen-2012-002112. Print 2013.
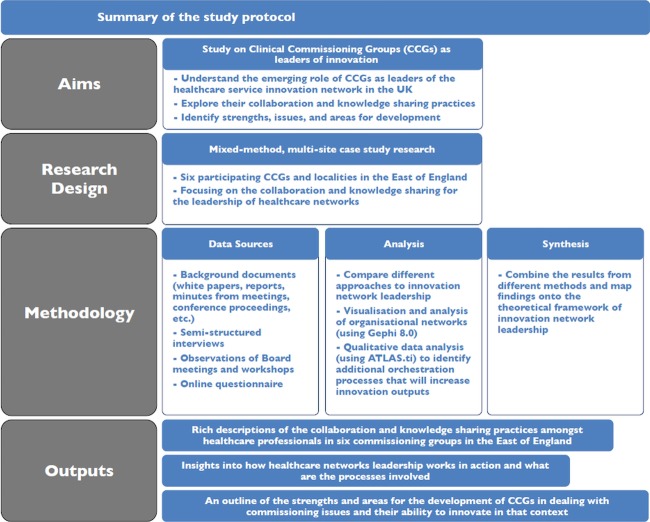
To explore the relational challenges for general practitioner (GP) leaders setting up new network-centric commissioning organisations in the recent health policy reform in England, we use innovation network theory to identify key network leadership practices that facilitate healthcare innovation.
Mixed-method, multisite and case study research.
Six clinical commissioning groups and local clusters in the East of England area, covering in total 208 GPs and 1 662 000 population.
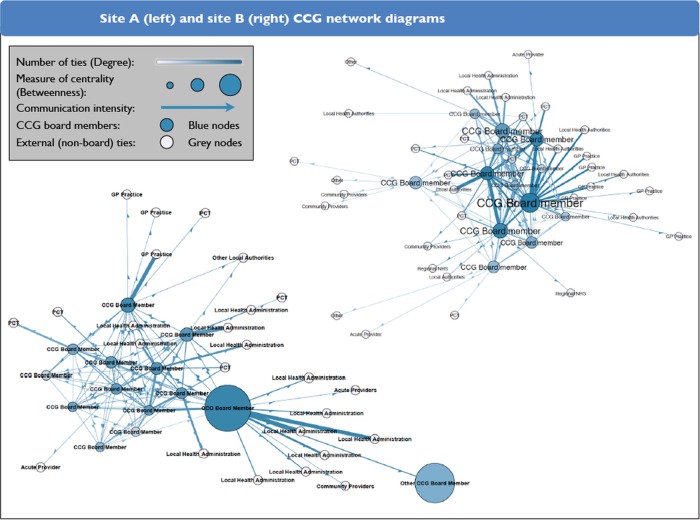
Semistructured interviews with 56 lead GPs, practice managers and staff from the local health authorities (primary care trusts, PCT) as well as various healthcare professionals; 21 observations of clinical commissioning group (CCG) board and executive meetings; electronic survey of 58 CCG board members (these included GPs, practice managers, PCT employees, nurses and patient representatives) and subsequent social network analysis.
Collaborative relationships between CCG board members and stakeholders from their healthcare network; clarifying the role of GPs as network leaders; strengths and areas for development of CCGs.
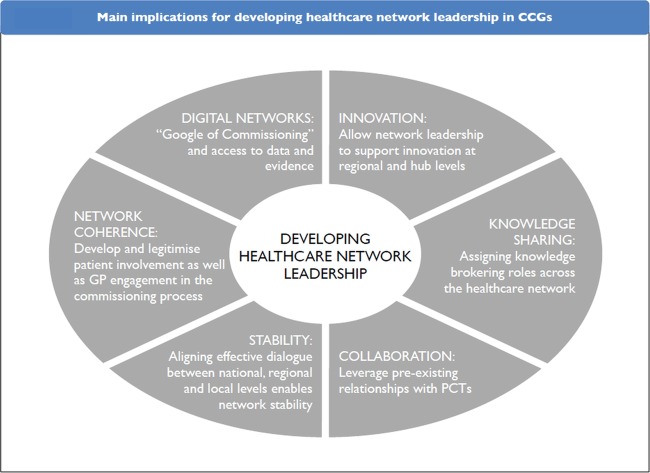
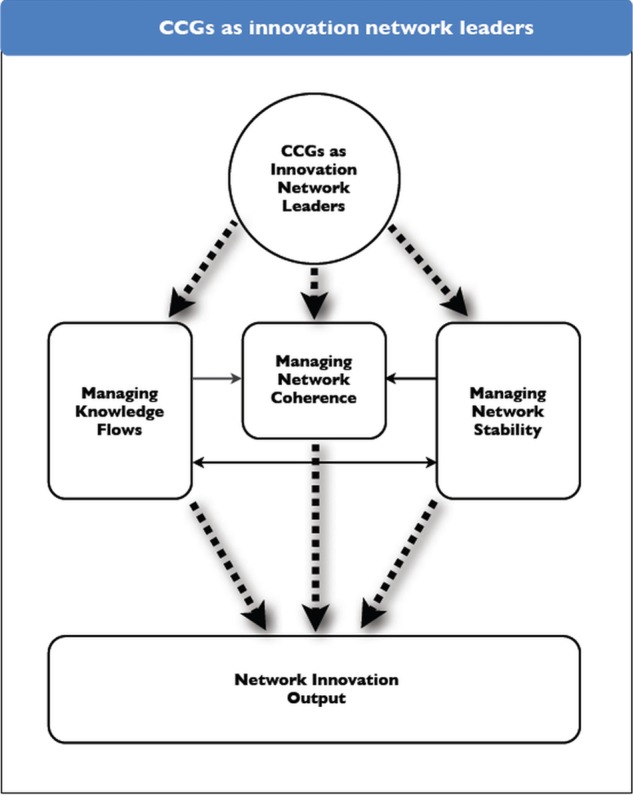
Drawing upon innovation network theory provides unique insights of the CCG leaders' activities in establishing best practices and introducing new clinical pathways. In this context we identified three network leadership roles: managing knowledge flows, managing network coherence and managing network stability. Knowledge sharing and effective collaboration among GPs enable network stability and the alignment of CCG objectives with those of the wider health system (network coherence). Even though activities varied between commissioning groups, collaborative initiatives were common. However, there was significant variation among CCGs around the level of engagement with providers, patients and local authorities. Locality (sub) groups played an important role because they linked commissioning decisions with patient needs and brought the leaders closer to frontline stakeholders.
With the new commissioning arrangements, the leaders should seek to move away from dyadic and transactional relationships to a network structure, thereby emphasising on the emerging relational focus of their roles. Managing knowledge mobility, healthcare network coherence and network stability are the three clinical leadership processes that CCG leaders need to consider in coordinating their network and facilitating the development of good clinical commissioning decisions, best practices and innovative services. To successfully manage these processes, CCG leaders need to leverage the relational capabilities of their network as well as their clinical expertise to establish appropriate collaborations that may improve the healthcare services in England. Lack of local GP engagement adds uncertainty to the system and increases the risk of commissioning decisions being irrelevant and inefficient from patient and provider perspectives.
利用创新网络理论,确定有利于医疗保健创新的关键网络领导实践,探索全科医生(GP)领导者在英国最近的卫生政策改革中建立新的以网络为中心的委托组织所面临的关系挑战。
混合方法、多地点和案例研究。
英格兰东部的六个临床委托小组和地方集群,共覆盖 208 名全科医生和 1662000 名居民。
对来自地方卫生当局(初级保健信托,PCT)的 56 名主要 GP、管理人员和工作人员以及各种医疗保健专业人员进行半结构化访谈;对 21 次临床委托小组(CCG)委员会和执行会议进行观察;对 58 名 CCG 委员会成员(包括全科医生、管理人员、PCT 员工、护士和患者代表)进行电子调查,随后进行社会网络分析。
CCG 委员会成员与他们的医疗网络利益相关者之间的协作关系;明确 GP 作为网络领导者的角色;CCG 的优势和发展领域。
借鉴创新网络理论,我们深入了解了 CCG 领导者在建立最佳实践和引入新临床途径方面的活动。在这种情况下,我们确定了三种网络领导角色:管理知识流、管理网络一致性和管理网络稳定性。GP 之间的知识共享和有效合作使网络稳定,并使 CCG 目标与更广泛的卫生系统(网络一致性)保持一致。尽管委托小组之间的活动有所不同,但协作举措很常见。然而,CCG 之间在与提供者、患者和地方当局的参与程度方面存在显著差异。地方(次)群体发挥了重要作用,因为它们将委托决策与患者需求联系起来,并使领导者更接近一线利益相关者。
随着新的委托安排,领导者应寻求从二元和交易关系转向网络结构,从而强调其角色的新兴关系焦点。管理知识流动性、医疗保健网络一致性和网络稳定性是 CCG 领导者在协调其网络和促进良好临床委托决策、最佳实践和创新服务发展时需要考虑的三个临床领导过程。为了成功管理这些过程,CCG 领导者需要利用其网络的关系能力以及他们的临床专业知识,建立适当的合作关系,从而可能改善英格兰的医疗保健服务。缺乏当地全科医生的参与给系统带来了不确定性,并增加了从患者和提供者的角度来看委托决策不相关和低效的风险。