The Nuffield Trust, London W1G 7LP, UK.
BMJ. 2011 Nov 22;343:d6608. doi: 10.1136/bmj.d6608.
To develop a formula for allocating resources for commissioning hospital care to all general practices in England based on the health needs of the people registered in each practice
Multivariate prospective statistical models were developed in which routinely collected electronic information from 2005-6 and 2006-7 on individuals and the areas in which they lived was used to predict their costs of hospital care in the next year, 2007-8. Data on individuals included all diagnoses recorded at any inpatient admission. Models were developed on a random sample of 5 million people and validated on a second random sample of 5 million people and a third sample of 5 million people drawn from a random sample of practices.
All general practices in England as of 1 April 2007. All NHS inpatient admissions and outpatient attendances for individuals registered with a general practice on that date.
All individuals registered with a general practice in England at 1 April 2007.
Power of the statistical models to predict the costs of the individual patient or each practice's registered population for 2007-8 tested with a range of metrics (R(2) reported here). Comparisons of predicted costs in 2007-8 with actual costs incurred in the same year were calculated by individual and by practice.
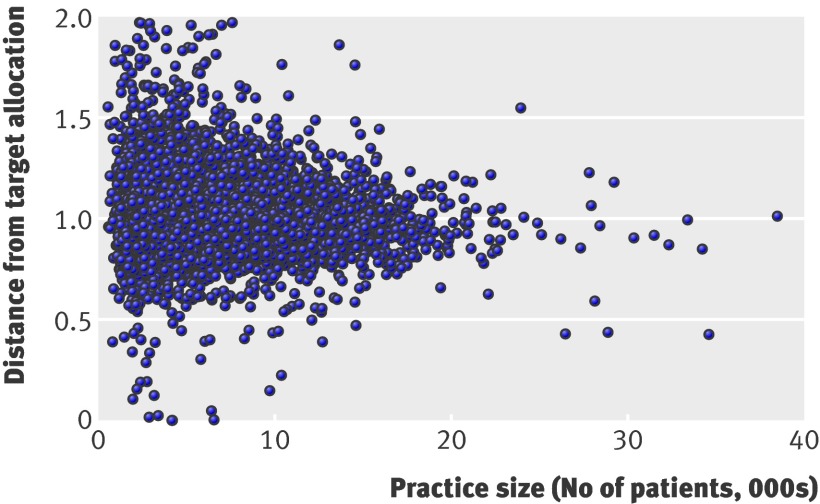
Models including person level information (age, sex, and ICD-10 codes diagnostic recorded) and a range of area level information (such as socioeconomic deprivation and supply of health facilities) were most predictive of costs. After accounting for person level variables, area level variables added little explanatory power. The best models for resource allocation could predict upwards of 77% of the variation in costs at practice level, and about 12% at the person level. With these models, the predicted costs of about a third of practices would exceed or undershoot the actual costs by 10% or more. Smaller practices were more likely to be in these groups.
A model was developed that performed well by international standards, and could be used for allocations to practices for commissioning. The best formulas, however, could predict only about 12% of the variation in next year's costs of most inpatient and outpatient NHS care for each individual. Person-based diagnostic data significantly added to the predictive power of the models.
根据登记在每个实践中的人群的健康需求,为英格兰所有的一般实践制定分配资源用于委托医院护理的方案。
在 2005-6 年和 2006-7 年期间,针对个体及其居住地区的常规收集的电子信息被用于预测他们在 2007-8 年的下一年的医院护理成本。个体的数据包括所有在住院治疗时记录的诊断。模型在随机抽取的 500 万人的样本上进行开发,并在另外 500 万人的随机样本和从实践中随机抽取的 500 万人的样本上进行验证。
截至 2007 年 4 月 1 日的英格兰所有一般实践。所有 NHS 住院和门诊就诊的个体登记在该日期的一般实践中。
2007 年 4 月 1 日在英格兰注册的所有个体。
使用一系列指标(此处报告的 R²)测试预测个体患者或每个实践注册人群的成本的统计模型的能力。通过个体和实践来计算 2007-8 年预测成本与同年实际成本之间的比较。
包含个人信息(年龄、性别和 ICD-10 诊断记录的代码)和一系列地区信息(如社会经济贫困和卫生设施供应)的模型对成本的预测能力最强。在考虑个人变量后,地区变量增加了很少的解释能力。资源分配的最佳模型可以预测实践水平上 77%以上的成本变化,以及个人水平上约 12%的成本变化。使用这些模型,大约三分之一的实践的预测成本将超过或低于实际成本 10%或更多。较小的实践更有可能属于这些群体。
开发了一种表现良好的模型,达到国际标准,并可用于向实践进行委托分配。然而,最好的公式只能预测大约 12%的大多数 NHS 住院和门诊护理的下一年个人成本变化。基于人的诊断数据显著增加了模型的预测能力。