Department of Colorectal Cancer Surgery, The 2nd Affiliated Hospital, Harbin Medical University, Harbin, Heilongjiang, China.
PLoS One. 2013;8(2):e56205. doi: 10.1371/journal.pone.0056205. Epub 2013 Feb 18.
The epidermal growth factor receptor (EGFR) gene copy number (GCN) has been previously demonstrated to correlate with the clinical outcome of colorectal cancer (CRC) treated with anti-EGFR monoclonal antibodies (mAbs), although it remains controversial. We conducted a systematic review and meta-analysis to assess EGFR GCN as a potential biomarker of survival for patients with advanced CRC receiving treatment with anti-EGFR mAbs.
We systematically identified articles investigating EGFR GCN by fluorescent or chromogenic in situ hybridization or other detection techniques in patients with metastatic CRC treated with panitumumab or cetuximab, (last search: 10 August 2012). Eligible studies had to report on overall survival (OS), progression-free survival (PFS) or time-to-progression (TTP), stratified by EGFR GCN. Summary hazard ratios (HRs) were calculated using random-effects models.
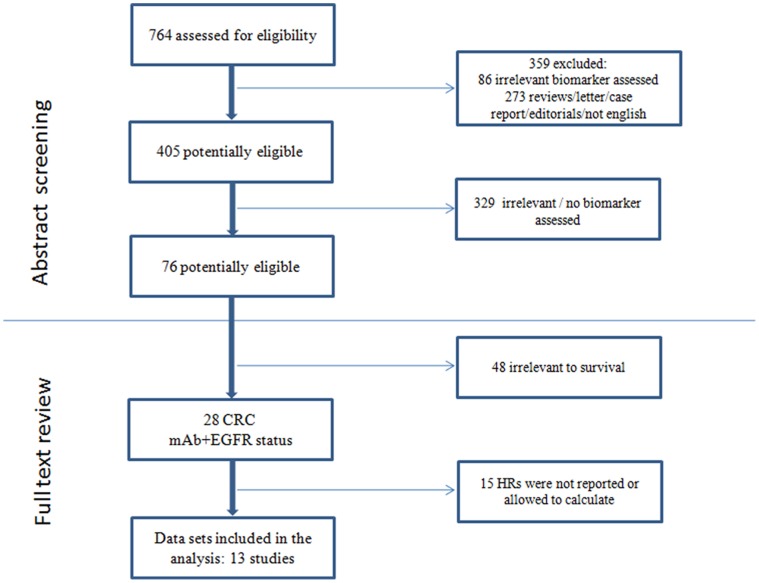
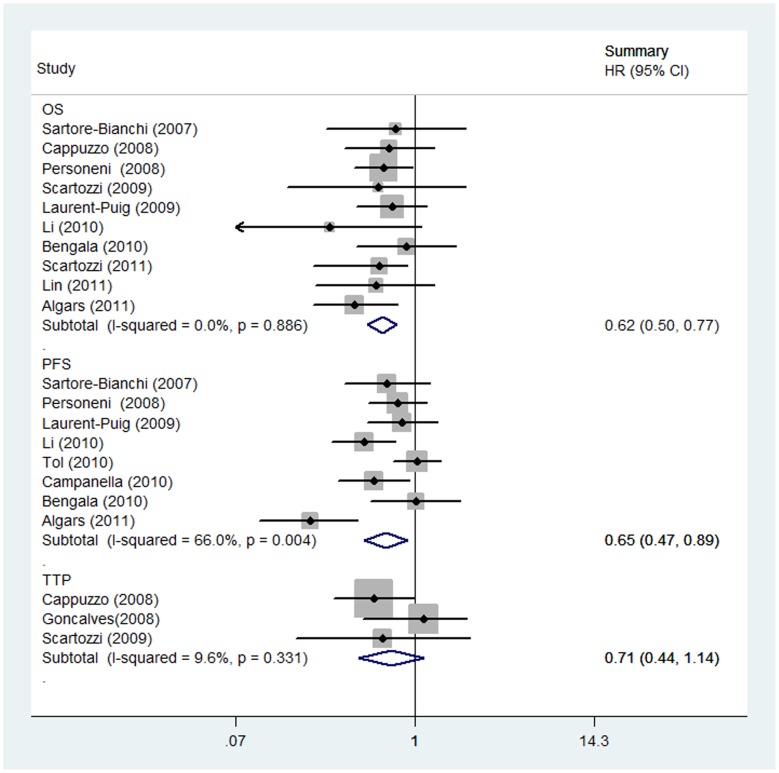
Among 13 identified studies, 10 (776 patients, 302 with increased GCN), 8 (893 patients, 282 with increased GCN) and 3 (149 patients, 66 with increased GCN) were eligible for the OS, PFS and TTP meta-analyses, respectively. Increased EGFR GCN was associated with increased OS (HR = 0.62; 95% CI 0.50-0.77; P<0.001), PFS (HR = 0.65; 95% CI 0.47-0.89; P = 0.008) but not TTP (HR = 0.71; 95% CI 0.44-1.14; P = 0.157). It was also shown that EGFR GCN is independent of other factors such as KRAS status. Among those populations received second-line or higher treatment, increased EGFR GCN was strongly associated with improved survival (for OS, HR = 0.60; 95% CI 0.47-0.75; P<0.001; for PFS, HR = 0.59; 95% CI 0.47-0.75; P<0.001), whereas it did not influence survival in patients that received first-line therapy.
Among the anti-EGFR-treated patients, increased EGFR GCN appears to be associated with improved survival outcomes. The effect on survival appears to be related to patients receiving the line of treatment.
表皮生长因子受体(EGFR)基因拷贝数(GCN)已被证明与接受抗 EGFR 单克隆抗体(mAb)治疗的结直肠癌(CRC)的临床结局相关,尽管这仍然存在争议。我们进行了一项系统评价和荟萃分析,以评估 EGFR GCN 作为接受抗 EGFR mAb 治疗的晚期 CRC 患者生存的潜在生物标志物。
我们通过荧光或显色原位杂交或其他检测技术系统地鉴定了研究 EGFR GCN 的文章,这些文章涉及接受 panitumumab 或 cetuximab 治疗的转移性 CRC 患者(最后一次搜索:2012 年 8 月 10 日)。符合条件的研究必须报告总体生存(OS)、无进展生存(PFS)或进展时间(TTP),按 EGFR GCN 分层。使用随机效应模型计算汇总危险比(HR)。
在 13 项确定的研究中,10 项(776 名患者,302 名 EGFR GCN 升高)、8 项(893 名患者,282 名 EGFR GCN 升高)和 3 项(149 名患者,66 名 EGFR GCN 升高)分别符合 OS、PFS 和 TTP 荟萃分析的条件。增加的 EGFR GCN 与 OS 增加相关(HR=0.62;95%CI 0.50-0.77;P<0.001)、PFS(HR=0.65;95%CI 0.47-0.89;P=0.008)但与 TTP 无关(HR=0.71;95%CI 0.44-1.14;P=0.157)。还表明,EGFR GCN 独立于 KRAS 状态等其他因素。在接受二线或更高线治疗的人群中,增加的 EGFR GCN 与生存改善密切相关(OS,HR=0.60;95%CI 0.47-0.75;P<0.001;PFS,HR=0.59;95%CI 0.47-0.75;P<0.001),而在接受一线治疗的患者中,EGFR GCN 并不影响生存。
在接受抗 EGFR 治疗的患者中,增加的 EGFR GCN 似乎与改善的生存结果相关。这种对生存的影响似乎与接受治疗的患者有关。