Institute for Hygiene and Microbiology, University of Würzburg, Josef Schneider-Strasse 2, Würzburg, 97080, Germany.
BMC Infect Dis. 2013 Feb 28;13:111. doi: 10.1186/1471-2334-13-111.
Published models predicting nasal colonization with Methicillin-resistant Staphylococcus aureus among hospital admissions predominantly focus on separation of carriers from non-carriers and are frequently evaluated using measures of discrimination. In contrast, accurate estimation of carriage probability, which may inform decisions regarding treatment and infection control, is rarely assessed. Furthermore, no published models adjust for MRSA prevalence.
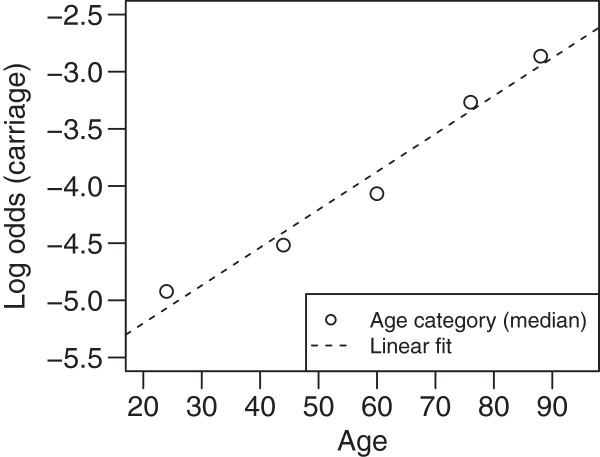
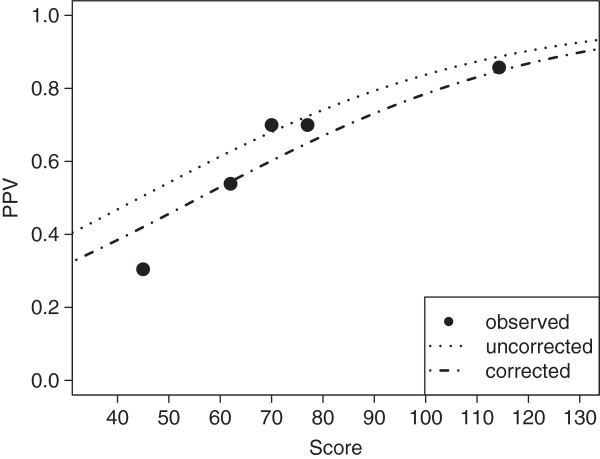
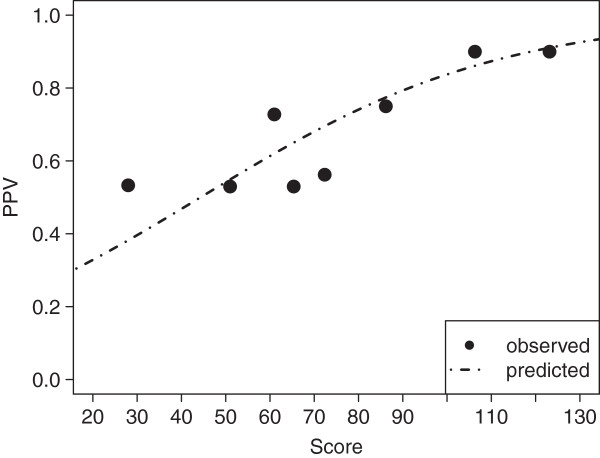
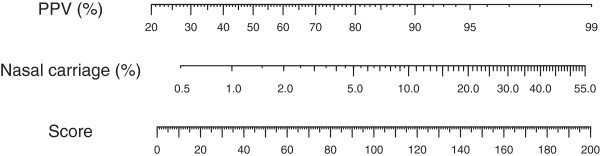
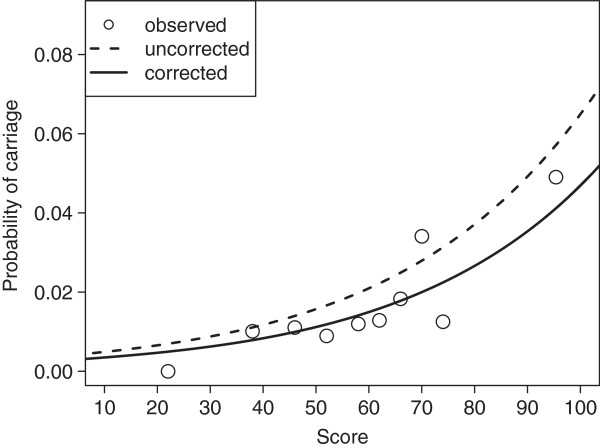
Using logistic regression, a scoring system (values from 0 to 200) predicting nasal carriage of MRSA was created using a derivation cohort of 3091 individuals admitted to a European tertiary referral center between July 2007 and March 2008. The expected positive predictive value of a rapid diagnostic test (GeneOhm, Becton & Dickinson Co.) was modeled using non-linear regression according to score. Models were validated on a second cohort from the same hospital consisting of 2043 patients admitted between August 2008 and January 2012. Our suggested correction score for prevalence was proportional to the log-transformed odds ratio between cohorts. Calibration before and after correction, i.e. accurate classification into arbitrary strata, was assessed with the Hosmer-Lemeshow-Test.
Treating culture as reference, the rapid diagnostic test had positive predictive values of 64.8% and 54.0% in derivation and internal validation corhorts with prevalences of 2.3% and 1.7%, respectively. In addition to low prevalence, low positive predictive values were due to high proportion (> 66%) of mecA-negative Staphylococcus aureus among false positive results. Age, nursing home residence, admission through the medical emergency department, and ICD-10-GM admission diagnoses starting with "A" or "J" were associated with MRSA carriage and were thus included in the scoring system, which showed good calibration in predicting probability of carriage and the rapid diagnostic test's expected positive predictive value. Calibration for both probability of carriage and expected positive predictive value in the internal validation cohort was improved by applying the correction score.
Given a set of patient parameters, the presented models accurately predict a) probability of nasal carriage of MRSA and b) a rapid diagnostic test's expected positive predictive value. While the former can inform decisions regarding empiric antibiotic treatment and infection control, the latter can influence choice of screening method.
已发表的预测耐甲氧西林金黄色葡萄球菌(MRSA)定植的模型主要集中在对定植者和非定植者的分离上,并且经常使用区分度来评估。相比之下,对定植概率的准确估计很少被评估,而定植概率的估计可能会影响关于治疗和感染控制的决策。此外,没有发表的模型可以调整 MRSA 的流行率。
使用逻辑回归,创建了一个评分系统(分值范围为 0 至 200),以预测 2007 年 7 月至 2008 年 3 月期间入住欧洲三级转诊中心的 3091 名个体的鼻腔携带 MRSA 的情况。根据评分,使用非线性回归来模拟快速诊断测试(GeneOhm,Becton & Dickinson Co.)的预期阳性预测值。根据评分,使用来自同一医院的第二个队列(2008 年 8 月至 2012 年 1 月期间入院的 2043 名患者)对模型进行验证。我们建议的流行率校正评分与队列之间的对数转换比值成正比。通过 Hosmer-Lemeshow 检验评估校正前后的校准,即任意分层的准确分类。
以培养物为参考,快速诊断测试在具有 2.3%和 1.7%流行率的衍生队列和内部验证队列中的阳性预测值分别为 64.8%和 54.0%。除了低流行率外,阳性预测值低还归因于假阳性结果中 mecA 阴性金黄色葡萄球菌的比例(>66%)较高。年龄、疗养院居住、通过急诊部入院以及以“ A”或“ J”开头的 ICD-10-GM 入院诊断与 MRSA 定植相关,因此被纳入评分系统,该系统在预测定植概率和快速诊断测试的预期阳性预测值方面显示出良好的校准。在内部验证队列中,通过应用校正评分,对定植概率和预期阳性预测值的校准都得到了改善。
在给定一组患者参数的情况下,本研究提供的模型可准确预测 a)MRSA 鼻腔定植的概率,b)快速诊断测试的预期阳性预测值。前者可以为经验性抗生素治疗和感染控制的决策提供信息,后者可以影响筛查方法的选择。