Division of Pediatric Cardiology, Department of Pediatrics, Stanford University, Palo Alto, California 94304, USA.
J Heart Lung Transplant. 2013 May;32(5):546-52. doi: 10.1016/j.healun.2013.01.1055. Epub 2013 Feb 28.
Pediatric patients with severe pulmonary arterial hypertension (PAH) are treated with intravenous epoprostenol or intravenous or subcutaneous treprostinil. Little is known about longitudinal hemodynamics and outcomes of epoprostenol, treprostinil, and transitions from epoprostenol to treprostinil.
This was retrospective study of 77 pediatric patients (47 idiopathic PAH, 24 congenital heart disease-PAH) receiving epoprostenol or treprostinil from 1992 to 2010 at 2 centers. Outcomes were defined as living vs dead/transplant.
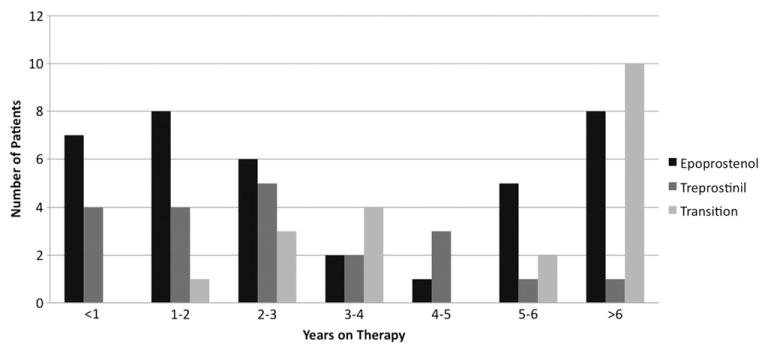
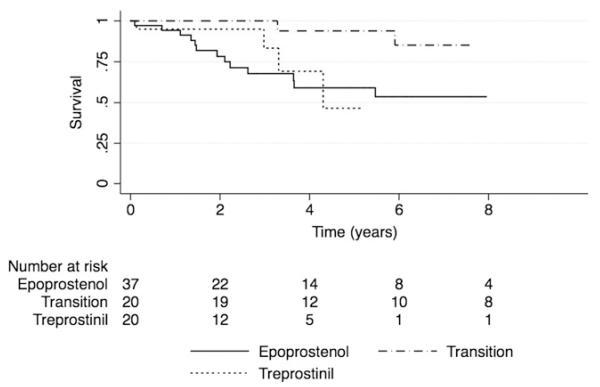
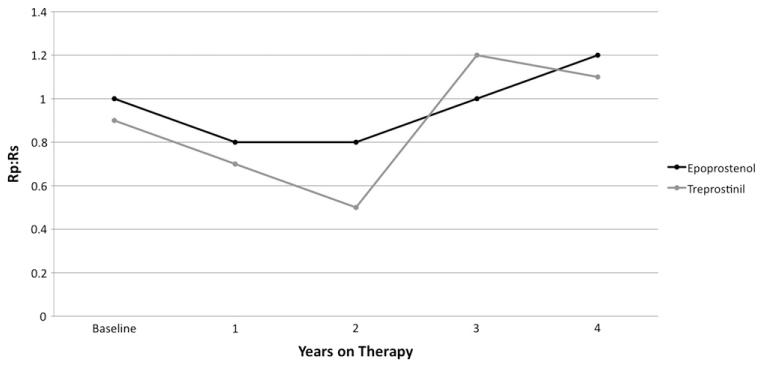
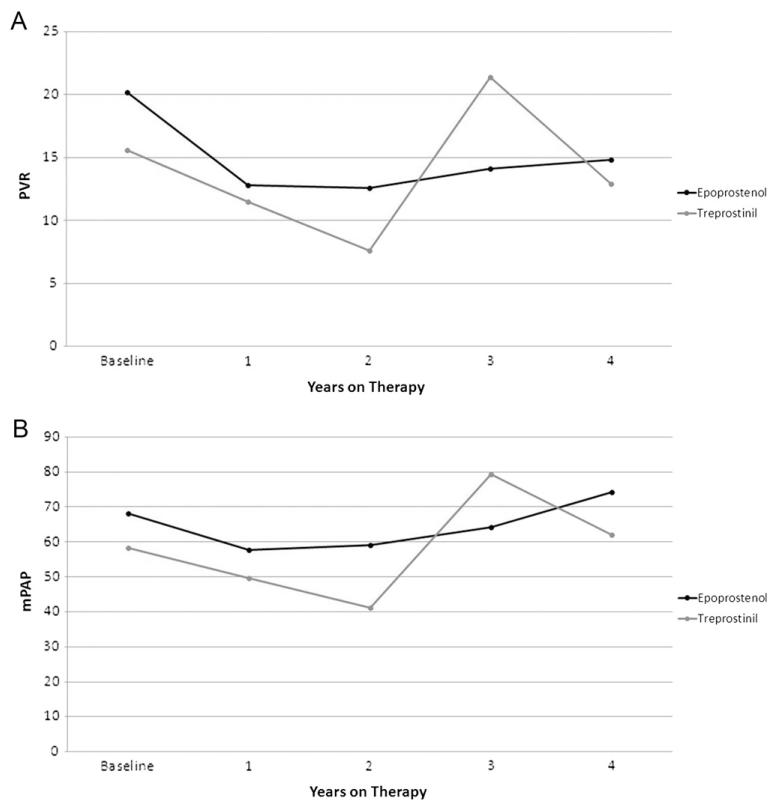
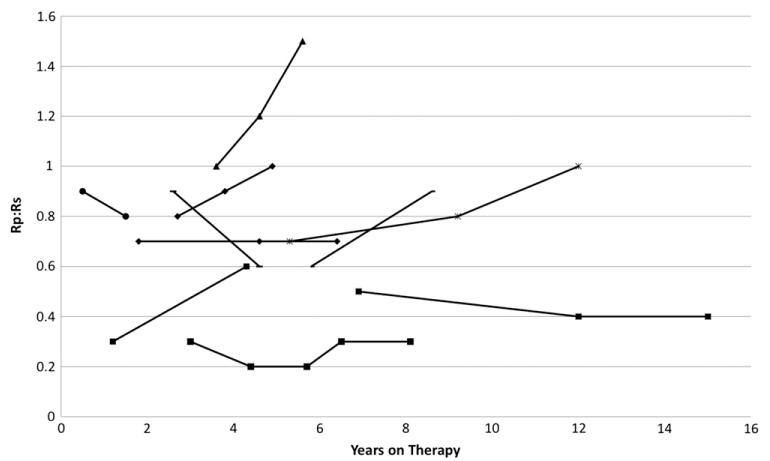
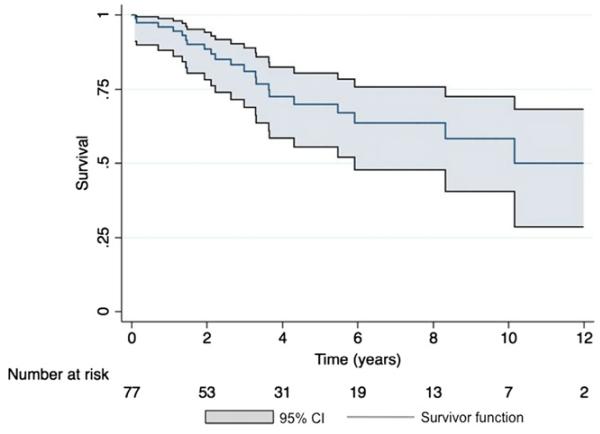
Mean age at baseline was 7.7 ± 5.2 years, with follow-up of 4.3 ± 3.4 years. Thirty-seven patients were treated with epoprostenol, 20 with treprostinil, and 20 were transitioned from epoprostenol to treprostinil. Mean pulmonary-to-systemic vascular resistance ratio (Rp/Rs) for epoprostenol was 1.0 ± 0.4, 0.8 ± 0.4, 0.8 ± 0.4, 1.0 ± 0.4, and 1.2 ± 0.4, respectively, at baseline, 1, 2, 3, and 4 years. For treprostinil, Rp/Rs was 0.9 ± 0.3, 0.7 ± 0.3, 0.5 ± 0.2, (p < 0.01 vs baseline), and 1.1 ± 0.2, respectively, at baseline, 1, 2, and 3 to 4 years, respectively. There were similar changes in mean pulmonary artery pressure and pulmonary vascular resistance index. The Rp/Rs 1 year after epoprostenol to treprostinil transition increased from 0.6 to 0.8 (n = 7). Changes not statistically significant unless noted. Eight patients died or received a transplant within 2 years of baseline; compared with the rest of the cohort, mean baseline Rp/Rs, right atrial pressure, and pulmonary vascular resistance index were significantly worse in this group. Thirty-nine patients remain on prostanoids, 17 are off, 16 died, and 5 received heart-lung transplant. Kaplan-Meier 5-year transplant-free survival was 70% (95% confidence interval, 56%-80%).
There was improvement in Rp/Rs on both therapies at 1 to 2 years that was not sustained. The 5-year transplant-free survival was better than in similar adult studies.
患有严重肺动脉高压(PAH)的儿科患者接受静脉内依前列醇或静脉内或皮下曲前列尼尔治疗。对于依前列醇、曲前列尼尔以及从依前列醇转换为曲前列尼尔的纵向血液动力学和结局,知之甚少。
这是一项回顾性研究,纳入了 1992 年至 2010 年在两个中心接受依前列醇或曲前列尼尔治疗的 77 名儿科患者(47 名特发性 PAH,24 名先天性心脏病-PAH)。结局定义为存活与死亡/移植。
基线时的平均年龄为 7.7 ± 5.2 岁,随访时间为 4.3 ± 3.4 年。37 名患者接受依前列醇治疗,20 名患者接受曲前列尼尔治疗,20 名患者从依前列醇转换为曲前列尼尔。依前列醇的肺-体循环血管阻力比(Rp/Rs)分别为基线时的 1.0 ± 0.4、1.0 ± 0.4、1.0 ± 0.4、1.0 ± 0.4 和 1.2 ± 0.4,1 年、2 年、3 年和 4 年。曲前列尼尔的 Rp/Rs 分别为基线时的 0.9 ± 0.3、0.7 ± 0.3、0.5 ± 0.2、(p < 0.01 与基线相比)和 1.1 ± 0.2,1 年、2 年和 3 至 4 年。平均肺动脉压和肺血管阻力指数均有类似的变化。依前列醇转换为曲前列尼尔后 1 年 Rp/Rs 从 0.6 增加到 0.8(n = 7)。除非另有说明,否则变化不具有统计学意义。8 名患者在基线后 2 年内死亡或接受了移植;与队列中的其余患者相比,该组的平均基线 Rp/Rs、右心房压和肺血管阻力指数明显更差。39 名患者仍在使用前列环素,17 名已停药,16 名死亡,5 名接受心肺移植。Kaplan-Meier 5 年无移植生存为 70%(95%置信区间,56%-80%)。
两种治疗方法在 1 至 2 年内 Rp/Rs 均有改善,但未持续。5 年无移植生存率优于类似的成人研究。