Massachusetts General Hospital, Division of Infectious Disease, Center for Global Health, Boston, Massachusetts, USA.
PLoS One. 2013;8(3):e56400. doi: 10.1371/journal.pone.0056400. Epub 2013 Mar 5.
Antiretroviral prophylaxis may be a critical strategy to reduce periconception HIV transmission. Maximizing the benefit of periconception pharmacologic HIV risk-reduction requires an understanding of the links between pregnancy and adherence to this prevention strategy.
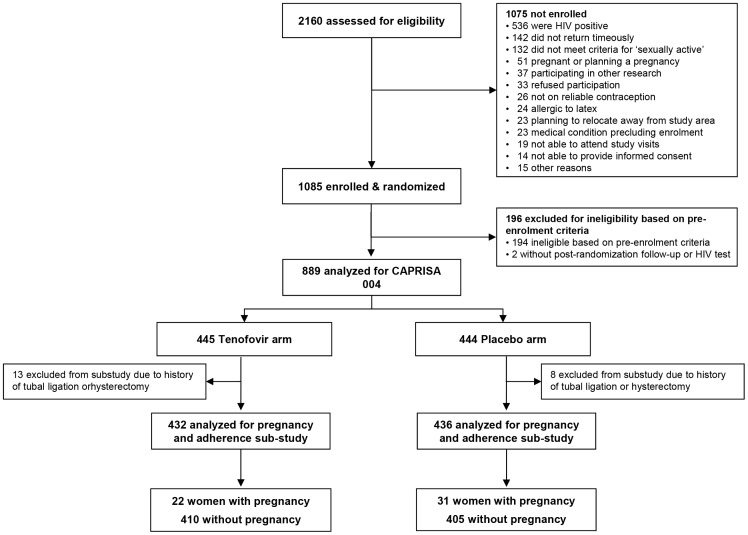
We assessed study gel adherence among women with pregnancies compared to women without pregnancies enrolled in the CAPRISA 004 phase IIB trial of 1% vaginal tenofovir gel. Pregnancy was assessed with monthly urine tests. Adherence was measured monthly and defined as proportion of sex acts covered by two returned, used applicators based on pre- and post-coital dosing. High adherence was defined as a median adherence score of >80%, that is, more than 80% of sex acts were covered by two applications of study gel. A multivariate generalized estimating equations (GEE) model with a binomial distribution was used to assess covariates associated with high adherence (>80%) over time. Median adherence before and after pregnancy was compared using Wilcoxon signed rank test.
Among 868 women, 53 had at least 1 pregnancy (4.06 per 100 woman years, 95% CI: 3.04, 5.31). Women with pregnancies had lower median adherence compared to women without pregnancies (50% [IQR: 45-83] vs. 60% [IQR: 50-100], p = 0.02). Women with pregnancies also had a 48% lower odds of high adherence compared to women without pregnancies when adjusting for confounders (aOR 0.52, 95%CI: 0.41-0.66, p<0.0001). Among women with pregnancies, adherence before and after pregnancy was not different (50% [IQR: 46-83] vs. 55% [IQR: 20-100], p = 0.68).
Women with pregnancies were less likely to have high adherence to study gel compared to women without pregnancies. Understanding these differences may inform findings from HIV prevention trials and future implementation of antiretroviral prophylaxis for at-risk women who choose to conceive. The protocol for the parent trial is registered on ClinicalTrials.gov, NCT00441298, http://www.clinicaltrials.gov/ct2/show/NCT00441298.
抗逆转录病毒预防可能是减少围孕期 HIV 传播的关键策略。为了最大限度地提高围孕期药物降低 HIV 风险的益处,需要了解怀孕与遵循这种预防策略之间的联系。
我们评估了在 CAPRISA 004 二期 B 试验中,与未怀孕的女性相比,怀孕女性使用 1%阴道用替诺福韦凝胶的情况。通过每月尿液检测来评估怀孕情况。每月评估一次依从性,根据性交前后的剂量计算出用两个已用、已归还的阴道用药器覆盖的性行为比例。高依从性定义为中值依从性评分>80%,即 80%以上的性行为都使用了研究凝胶。采用二项分布的广义估计方程(GEE)模型评估随时间推移与高依从性(>80%)相关的协变量。使用 Wilcoxon 符号秩检验比较怀孕前后的中值依从性。
在 868 名女性中,有 53 名至少有一次怀孕(每 100 名女性 4.06 次,95%CI:3.04,5.31)。与未怀孕的女性相比,怀孕的女性中值依从性较低(50%[IQR:45-83]与 60%[IQR:50-100],p=0.02)。调整混杂因素后,与未怀孕的女性相比,怀孕的女性发生高依从性的可能性低 48%(调整后的优势比[OR]0.52,95%CI:0.41-0.66,p<0.0001)。在怀孕的女性中,怀孕前后的依从性没有差异(50%[IQR:46-83]与 55%[IQR:20-100],p=0.68)。
与未怀孕的女性相比,怀孕的女性使用研究凝胶的高依从性较低。了解这些差异可能会影响 HIV 预防试验的结果,并为选择怀孕的高危女性提供抗逆转录病毒预防措施的未来实施提供信息。该试验的方案已在 ClinicalTrials.gov 注册,NCT00441298,http://www.clinicaltrials.gov/ct2/show/NCT00441298。