Price Joan T, Wheeler Stephanie B, Stranix-Chibanda Lynda, Hosek Sybil G, Watts D Heather, Siberry George K, Spiegel Hans M L, Stringer Jeffrey S, Chi Benjamin H
*Division of Global Women's Health, Department of Obstetrics and Gynecology, University of North Carolina Chapel Hill, Chapel Hill, NC; †Department of Health Policy and Management, University of North Carolina at Chapel Hill, Chapel Hill, NC; ‡Department of Pediatrics and Child Health, College of Health Sciences, University of Zimbabwe, Harare, Zimbabwe; §Department of Psychiatry, John Stroger Hospital of Cook County, Chicago, IL; ‖Office of the Global AIDS Coordinator and Health Diplomacy, U.S. Department of State, Washington, DC; ¶Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, MD; and #Kelly Government Services, Contractor to Prevention Sciences Program, Division of AIDS, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD.
J Acquir Immune Defic Syndr. 2016 Aug 1;72 Suppl 2(Suppl 2):S145-53. doi: 10.1097/QAI.0000000000001063.
Antiretroviral pre-exposure prophylaxis (PrEP) for the prevention of HIV acquisition is cost-effective when delivered to those at substantial risk. Despite a high incidence of HIV infection among pregnant and breastfeeding women in sub-Saharan Africa (SSA), a theoretical increased risk of preterm birth on PrEP could outweigh the HIV prevention benefit.
We developed a decision analytic model to evaluate a strategy of daily oral PrEP during pregnancy and breastfeeding in SSA. We approached the analysis from a health care system perspective across a lifetime time horizon. Model inputs were derived from existing literature and local sources. The incremental cost-effectiveness ratio (ICER) of PrEP versus no PrEP was calculated in 2015 U.S. dollars per disability-adjusted life year (DALY) averted. We evaluated the effect of uncertainty in baseline estimates through one-way and probabilistic sensitivity analyses.
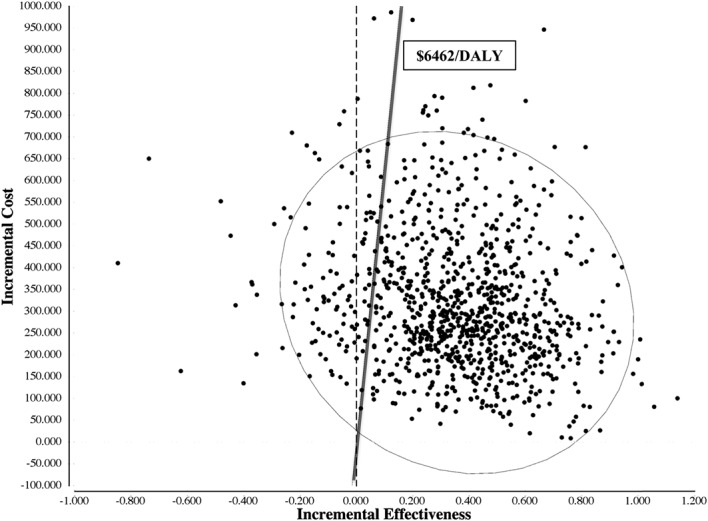
PrEP administered to pregnant and breastfeeding women in SSA was cost-effective. In a base case of 10,000 women, the administration of PrEP averted 381 HIV infections but resulted in 779 more preterm births. PrEP was more costly per person ($450 versus $117), but resulted in fewer disability-adjusted life years (DALYs) (3.15 versus 3.49). The incremental cost-effectiveness ratio of $965/DALY averted was below the recommended regional threshold for cost-effectiveness of $6462/DALY. Probabilistic sensitivity analyses demonstrated robustness of the model.
Providing PrEP to pregnant and breastfeeding women in SSA is likely cost-effective, although more data are needed about adherence and safety. For populations at high risk of HIV acquisition, PrEP may be considered as part of a broader combination HIV prevention strategy.
对于感染风险较高的人群,采用抗逆转录病毒药物暴露前预防(PrEP)来预防艾滋病毒感染具有成本效益。尽管撒哈拉以南非洲地区(SSA)的孕妇和哺乳期妇女艾滋病毒感染率很高,但PrEP理论上增加的早产风险可能会超过预防艾滋病毒的益处。
我们开发了一个决策分析模型,以评估在SSA地区对孕妇和哺乳期妇女采用每日口服PrEP的策略。我们从医疗保健系统的角度,在整个生命周期内进行分析。模型输入数据来自现有文献和当地资料。PrEP与不采用PrEP的增量成本效益比(ICER)以2015年美元计算,单位为每避免一个伤残调整生命年(DALY)。我们通过单因素和概率敏感性分析评估了基线估计值不确定性的影响。
在SSA地区对孕妇和哺乳期妇女使用PrEP具有成本效益。在10000名妇女的基础案例中,使用PrEP可避免381例艾滋病毒感染,但导致早产增加779例。PrEP每人成本更高(450美元对117美元),但导致的伤残调整生命年(DALY)更少(3.15对3.49)。每避免一个DALY的增量成本效益比为965美元,低于推荐的地区成本效益阈值6462美元/DALY。概率敏感性分析表明该模型具有稳健性。
在SSA地区为孕妇和哺乳期妇女提供PrEP可能具有成本效益,尽管还需要更多关于依从性和安全性的数据。对于艾滋病毒感染高危人群,PrEP可被视为更广泛的艾滋病毒综合预防策略的一部分。