Centre for Tropical Diseases, S. Cuore Hospital, Negrar, Verona, Italy.
PLoS One. 2013;8(3):e58019. doi: 10.1371/journal.pone.0058019. Epub 2013 Mar 5.
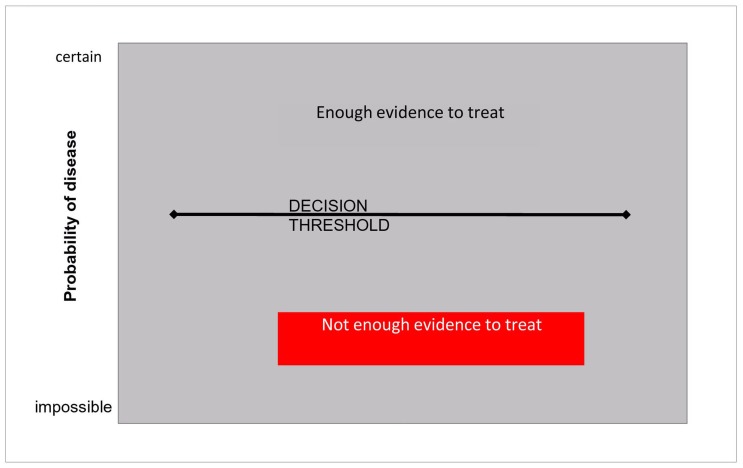
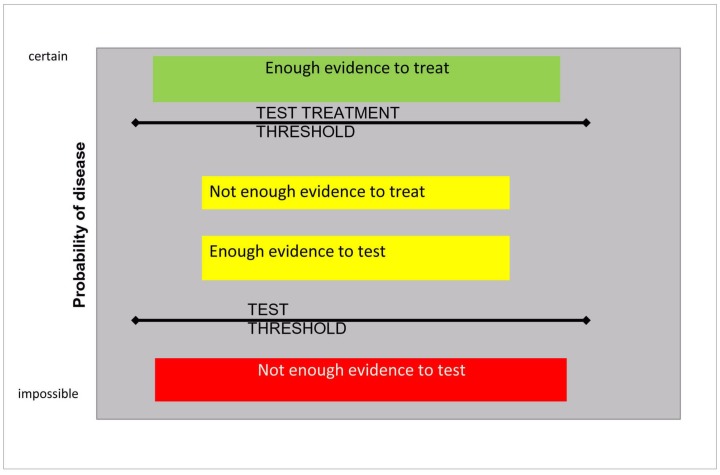
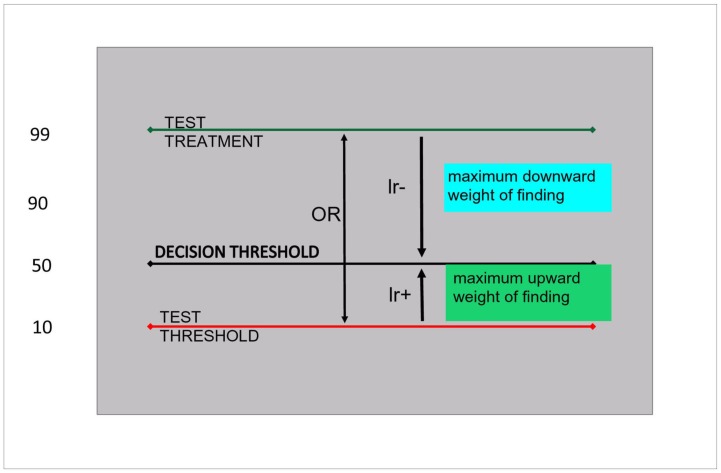
In Burkina Faso, rapid diagnostic tests for malaria have been made recently available. Previously, malaria was managed clinically. This study aims at assessing which is the best management option of a febrile patient in a hyperendemic setting. Three alternatives are: treating presumptively, testing, or refraining from both test and treatment. The test threshold is the tradeoff between refraining and testing, the test-treatment threshold is the tradeoff between testing and treating. Only if the disease probability lies between the two should the test be used.
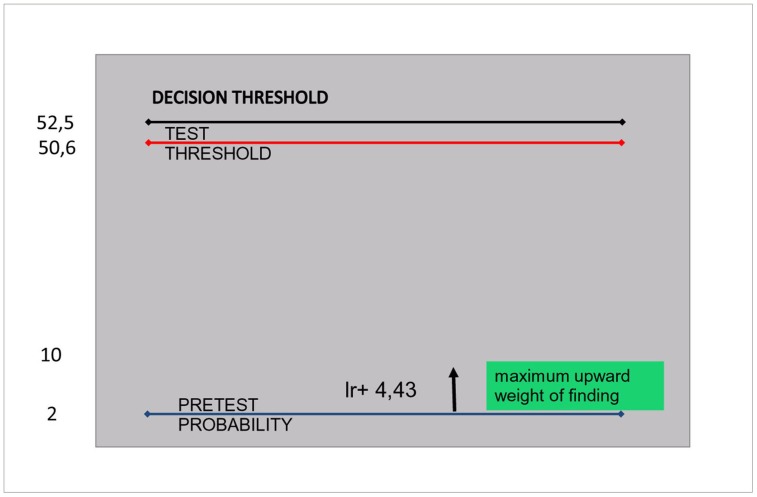
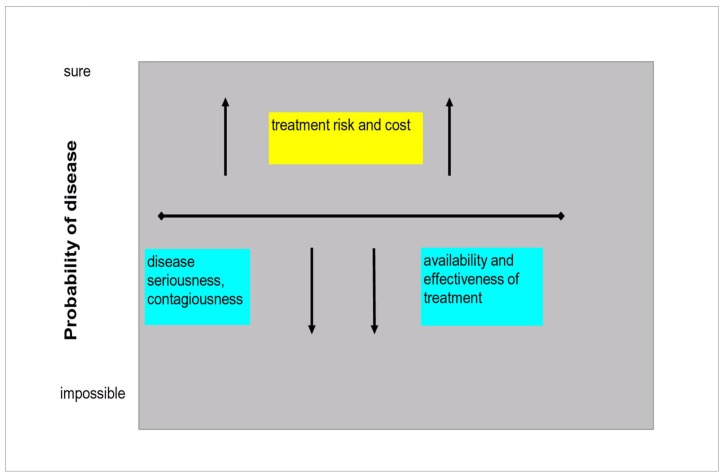
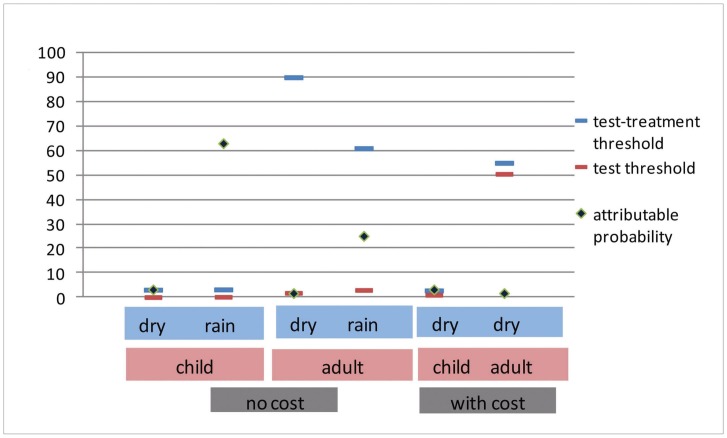
Data for this analysis was obtained from previous studies on malaria rapid tests, involving 5220 patients. The thresholds were calculated, based on disease risk, treatment risk and cost, test accuracy and cost. The thresholds were then matched against the disease probability. For a febrile child under 5 in the dry season, the pre-test probability of clinical malaria (3.2%), was just above the test/treatment threshold. In the rainy season, that probability was 63%, largely above the test/treatment threshold. For febrile children >5 years and adults in the dry season, the probability was 1.7%, below the test threshold, while in the rainy season it was higher (25.1%), and situated between the two thresholds (3% and 60.9%), only if costs were not considered. If they were, neither testing nor treating with artemisinin combination treatments (ACT) would be recommended.
A febrile child under 5 should be treated presumptively. In the dry season, the probability of clinical malaria in adults is so low, that neither testing nor treating with any regimen should be recommended. In the rainy season, if costs are considered, a febrile adult should not be tested, nor treated with ACT, but a possible alternative would be a presumptive treatment with amodiaquine plus sulfadoxine-pyrimethamine. If costs were not considered, testing would be recommended.
在布基纳法索,最近提供了快速诊断测试来检测疟疾。以前,疟疾是通过临床方法来治疗的。本研究旨在评估在高度流行地区,对发热患者的最佳管理方案。有三种选择:经验性治疗、检测或既不检测也不治疗。检测阈值是检测与不检测之间的权衡,检测-治疗阈值是检测与治疗之间的权衡。只有当疾病概率在两者之间时,才应该使用检测。
本分析的数据来自之前关于疟疾快速检测的研究,涉及 5220 名患者。根据疾病风险、治疗风险和成本、检测准确性和成本计算了阈值。然后将这些阈值与疾病概率进行匹配。对于 5 岁以下的干季发热儿童,临床疟疾的预检概率(3.2%)刚好高于检测-治疗阈值。在雨季,这个概率是 63%,大大高于检测-治疗阈值。对于 5 岁以上的发热儿童和成年人,在干季,概率为 1.7%,低于检测阈值,而在雨季,概率更高(25.1%),只有在不考虑成本的情况下,才处于检测-治疗阈值(3%和 60.9%)之间。如果考虑成本,则不建议进行检测或用青蒿素类复方疗法(ACT)进行治疗。
5 岁以下的发热儿童应进行经验性治疗。在干季,成年人患临床疟疾的概率非常低,不建议进行检测或任何治疗。在雨季,如果考虑成本,则不建议对发热成人进行检测或用 ACT 治疗,但可能的替代方案是用阿莫地喹加磺胺多辛-乙胺嘧啶进行经验性治疗。如果不考虑成本,则建议进行检测。