Division of Clinical Pharmacology and Toxicology, University Hospital Center and University of Lausanne, Lausanne, Switzerland.
PLoS One. 2011 Apr 8;6(4):e18578. doi: 10.1371/journal.pone.0018578.
Although CD4 cell count monitoring is used to decide when to start antiretroviral therapy in patients with HIV-1 infection, there are no evidence-based recommendations regarding its optimal frequency. It is common practice to monitor every 3 to 6 months, often coupled with viral load monitoring. We developed rules to guide frequency of CD4 cell count monitoring in HIV infection before starting antiretroviral therapy, which we validated retrospectively in patients from the Swiss HIV Cohort Study.
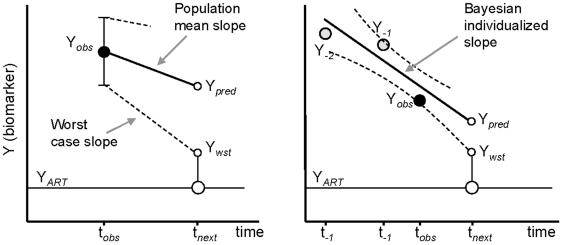
METHODOLOGY/PRINCIPAL FINDINGS: We built up two prediction rules ("Snap-shot rule" for a single sample and "Track-shot rule" for multiple determinations) based on a systematic review of published longitudinal analyses of CD4 cell count trajectories. We applied the rules in 2608 untreated patients to classify their 18 061 CD4 counts as either justifiable or superfluous, according to their prior ≥5% or <5% chance of meeting predetermined thresholds for starting treatment. The percentage of measurements that both rules falsely deemed superfluous never exceeded 5%. Superfluous CD4 determinations represented 4%, 11%, and 39% of all actual determinations for treatment thresholds of 500, 350, and 200×10(6)/L, respectively. The Track-shot rule was only marginally superior to the Snap-shot rule. Both rules lose usefulness for CD4 counts coming near to treatment threshold.
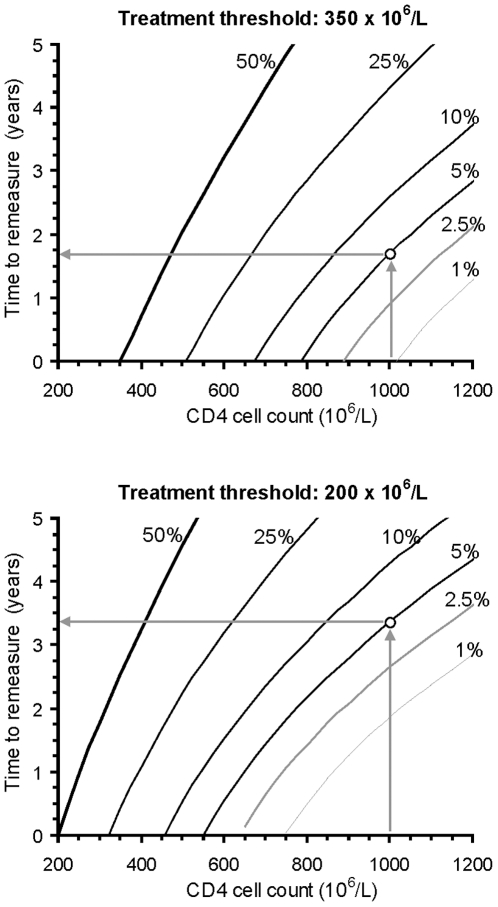
CONCLUSIONS/SIGNIFICANCE: Frequent CD4 count monitoring of patients with CD4 counts well above the threshold for initiating therapy is unlikely to identify patients who require therapy. It appears sufficient to measure CD4 cell count 1 year after a count >650 for a threshold of 200, >900 for 350, or >1150 for 500×10(6)/L, respectively. When CD4 counts fall below these limits, increased monitoring frequency becomes advisable. These rules offer guidance for efficient CD4 monitoring, particularly in resource-limited settings.
虽然 CD4 细胞计数监测用于决定何时开始对 HIV-1 感染患者进行抗逆转录病毒治疗,但关于其最佳频率尚无循证建议。通常的做法是每 3 至 6 个月监测一次,通常与病毒载量监测相结合。我们制定了在开始抗逆转录病毒治疗之前指导 HIV 感染中 CD4 细胞计数监测频率的规则,我们在瑞士艾滋病毒队列研究中的患者中进行了回顾性验证。
方法/主要发现:我们基于对 CD4 细胞计数轨迹的已发表纵向分析的系统回顾,建立了两个预测规则(“快照规则”用于单个样本和“轨迹规则”用于多个测定)。我们将这些规则应用于 2608 名未经治疗的患者,根据他们之前≥5%或<5%的机会达到预定的开始治疗阈值,将他们的 18061 个 CD4 计数分为合理或多余。两个规则都错误地认为多余的测量百分比从未超过 5%。对于治疗阈值为 500、350 和 200×10(6)/L 的所有实际测定值,多余的 CD4 测定值分别占 4%、11%和 39%。轨迹规则仅略优于快照规则。对于接近治疗阈值的 CD4 计数,两个规则的用处都不大。
结论/意义:频繁监测 CD4 计数明显高于开始治疗阈值的患者不太可能发现需要治疗的患者。对于阈值分别为 200×10(6)/L、350×10(6)/L 和 500×10(6)/L 的计数>650 后 1 年、>900 后 1 年和>1150 后 1 年测量 CD4 细胞计数似乎就足够了。当 CD4 计数低于这些限制时,增加监测频率是明智的。这些规则为高效的 CD4 监测提供了指导,特别是在资源有限的环境中。