Division of Transplant Surgery, University of Colorado Denver, Denver, CO 80045, USA.
Liver Transpl. 2013 Mar;19(3):259-67. doi: 10.1002/lt.23595.
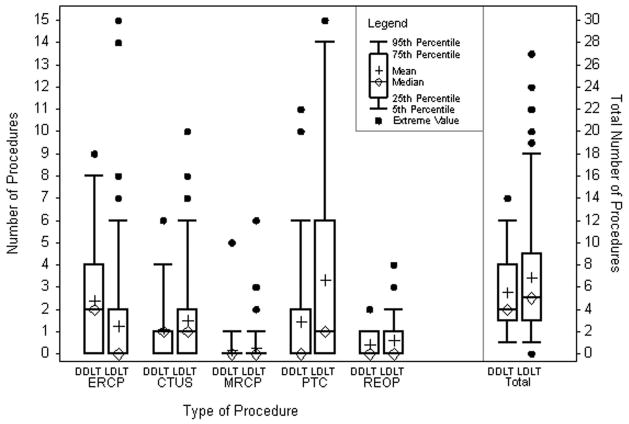
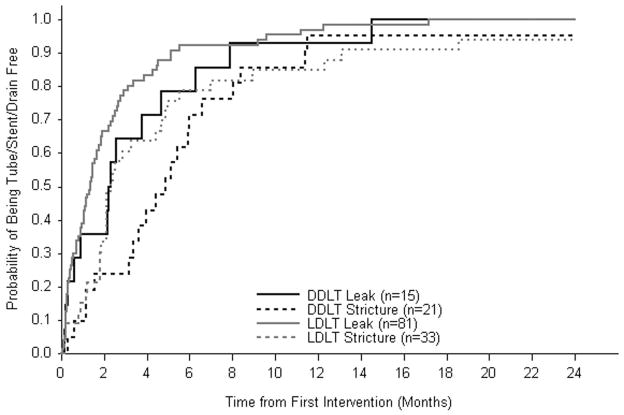
Adult recipients of living donor liver transplantation (LDLT) have a higher incidence of biliary complications than recipients of deceased donor liver transplantation (DDLT). Our objective was to define the intensity of the interventions and the time to resolution after the diagnosis of biliary complications after liver transplantation. We analyzed the management and resolution of posttransplant biliary complications and investigated the comparative effectiveness of interventions in LDLT and DDLT recipients. For the analysis of biliary complications (leaks or strictures), we used a retrospective cohort of patients who underwent liver transplantation at 8 centers between 1998 and 2006 (median follow-up from onset=4.7 years). The numbers, procedure types, and times to resolution were compared for LDLT and DDLT recipients. Posttransplant biliary complications occurred in 47 of the 189 DDLT recipients (25%) and in 141 of the 356 LDLT recipients (40%). Biliary leaks constituted 38% of the post-DDLT biliary complications (n=18) and 65% of the post-LDLT biliary complications (n=91). The median times to first biliary complications were similar for DDLT and LDLT (11 versus 14 days for leaks, P=0.63; 69 versus 107 days for strictures, P=0.34). Overall, 1225 diagnostic and therapeutic procedures, including reoperation and retransplantation, were performed (6.5±5.4 per recipient; 5.5±3.6 for DDLT versus 6.8±5.8 for LDLT, P=0.52). The median number of months to the resolution of a biliary complication (i.e., a tube-, stent-, and drain-free status) did not significantly differ between the DDLT and LDLT groups for leaks (2.3 versus 1.3 months, P=0.29) or strictures (4.9 versus 2.3 months, P=0.61). Although the incidence of biliary complications is higher after LDLT versus DDLT, the treatment requirements and the time to resolution after the development of a biliary complication are similar for LDLT and DDLT recipients.
成人活体肝移植(LDLT)受者的胆道并发症发生率高于尸肝移植(DDLT)受者。我们的目的是确定胆道并发症诊断后的干预强度和解决时间。我们分析了肝移植后胆道并发症的处理和解决情况,并研究了 LDLT 和 DDLT 受者干预措施的比较效果。对于胆道并发症(漏或狭窄)的分析,我们使用了 1998 年至 2006 年间在 8 个中心进行肝移植的患者回顾性队列(从发病开始的中位随访时间=4.7 年)。比较了 LDLT 和 DDLT 受者的数量、手术类型和解决时间。47 例 DDLT 受者(25%)和 141 例 LDLT 受者(40%)发生了移植后胆道并发症。胆道漏构成了 38%的 DDLT 后胆道并发症(n=18)和 65%的 LDLT 后胆道并发症(n=91)。DLT 和 LDLT 的首次胆道并发症的中位时间相似(漏的 11 天与 14 天,P=0.63;狭窄的 69 天与 107 天,P=0.34)。总的来说,进行了 1225 次诊断和治疗操作,包括再次手术和再次移植(每位受者 6.5±5.4 次;DLT 为 5.5±3.6 次,LDLT 为 6.8±5.8 次,P=0.52)。胆道并发症(即无管、无支架和无引流)解决的中位时间在 DDLT 和 LDLT 组之间没有显著差异,无论是漏还是狭窄(漏的 2.3 个月与 1.3 个月,P=0.29;狭窄的 4.9 个月与 2.3 个月,P=0.61)。尽管 LDLT 后的胆道并发症发生率高于 DDLT,但 LDLT 和 DDLT 受者发生胆道并发症后的治疗需求和解决时间相似。