Wahlberg Jeanette, Ekman Bertil
Section of Endocrinology, Department of Medicine and Health Sciences, Faculty of Health, Sciences, Linköping University, Linköping, Sweden.
J Med Case Rep. 2013 Mar 19;7:80. doi: 10.1186/1752-1947-7-80.
Pulmonary carcinoids associated with ectopic adrenocorticotropic hormone secretion have a good prognosis if histological examination shows typical pulmonary carcinoid and low proliferation, whereas a poor outcome is linked to atypical pulmonary carcinoid and high proliferation. Here we describe the diagnostic challenges to find the tumor in Cushing's syndrome secondary to ectopic adrenocorticotropic hormone secretion in two cases with an atypical and a typical pulmonary carcinoid, respectively.
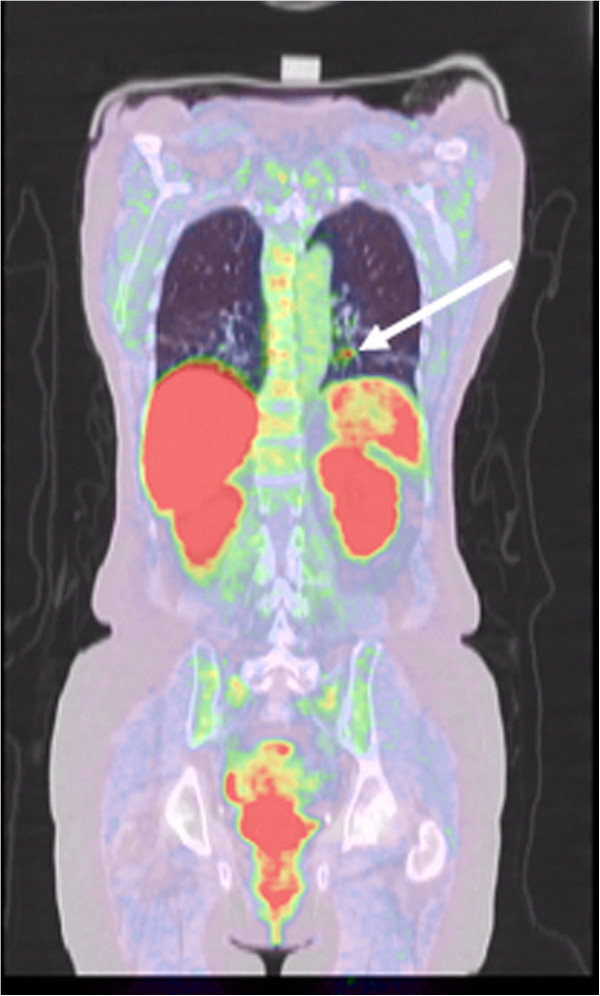
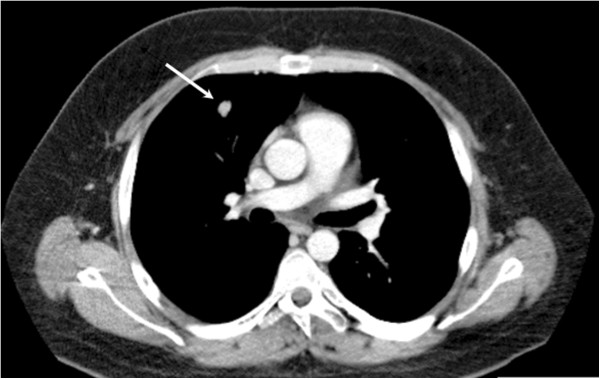
A 63-year-old Caucasian woman presented with aggressive clinical features related to Cushing's syndrome, having very high levels of urinary cortisol and circulating adrenocorticotropic hormone and cortisol. Magnetic resonance imaging showed no pituitary tumor, and bilateral inferior petrosal sinus sampling revealed no central peripheral ratio of adrenocorticotropic hormone. Computed tomography and 111Indium-pentetreoide somatostatin receptor scintigraphy could not visualize any ectopic tumor. The patient was referred for an 11C-5-hydroxytryptophan positron emission tomography, and a small 8mm nodule in her left lung was found. The tumor was removed via a lateral thoracic incision and wedge excision. The histological examination showed an atypical carcinoid with Ki-67 index of 9 to 10%, and an additional lobectomy was performed.The second patient, a 22-year-old Caucasian man, also presented with aggressive Cushing's syndrome, with very high urinary cortisol levels and increased circulating cortisol as well as adrenocorticotropic hormone levels. A magnetic resonance imaging scan of the pituitary showed no tumor, whereas a 12×9×14mm tumor was detected in the right lung on the primary computed tomography scan and no further investigation was performed. The tumor was removed via a lateral thoracic incision and wedge excision. A typical carcinoid with Ki-67 index of 1 to 2% was found and no further surgery was performed.After surgical removal, the biochemical disturbances resolved and significant clinical improvement were achieved in both patients after 24 months of follow up.
Diagnostic evaluation time is limited due to the aggressive course in ectopic adrenocorticotropic hormone-dependent Cushing's syndrome. We suggest that 11C-5-hydroxytryptophan positron emission tomography could be considered early as a secondary diagnostic tool when primary computed tomography and/or magnetic resonance imaging scans fail to show any tumor.
与异位促肾上腺皮质激素分泌相关的肺类癌,如果组织学检查显示为典型肺类癌且增殖率低,则预后良好,而不典型肺类癌和高增殖率则与不良预后相关。在此,我们描述了分别在两例不典型和典型肺类癌患者中,诊断继发于异位促肾上腺皮质激素分泌的库欣综合征肿瘤时所面临的挑战。
一名63岁的白种女性,表现出与库欣综合征相关的侵袭性临床特征,尿皮质醇、循环促肾上腺皮质激素和皮质醇水平极高。磁共振成像未显示垂体肿瘤,双侧岩下窦取样显示促肾上腺皮质激素无中央外周比值。计算机断层扫描和111铟-喷曲肽生长抑素受体闪烁显像均未发现任何异位肿瘤。该患者接受了11C-5-羟色氨酸正电子发射断层扫描,发现左肺有一个8毫米的小结节。通过侧胸切口和楔形切除术切除肿瘤。组织学检查显示为不典型类癌,Ki-67指数为9%至10%,随后进行了额外的肺叶切除术。第二名患者是一名22岁的白种男性,也表现出侵袭性库欣综合征,尿皮质醇水平极高,循环皮质醇以及促肾上腺皮质激素水平升高。垂体磁共振成像扫描未发现肿瘤,而在初次计算机断层扫描中发现右肺有一个12×9×14毫米的肿瘤,未进行进一步检查。通过侧胸切口和楔形切除术切除肿瘤。发现为典型类癌,Ki-67指数为1%至2%,未进行进一步手术。手术切除后,生化紊乱得到缓解,随访24个月后两名患者均有显著临床改善。
由于异位促肾上腺皮质激素依赖性库欣综合征病程侵袭性强,诊断评估时间有限。我们建议,当初次计算机断层扫描和/或磁共振成像扫描未能显示任何肿瘤时,可早期考虑将11C-5-羟色氨酸正电子发射断层扫描作为二级诊断工具。