Medical University Department, University of Basel, Kantonsspital Aarau, Tellstrasse, Aarau 5001, Switzerland.
Trials. 2013 Mar 22;14:84. doi: 10.1186/1745-6215-14-84.
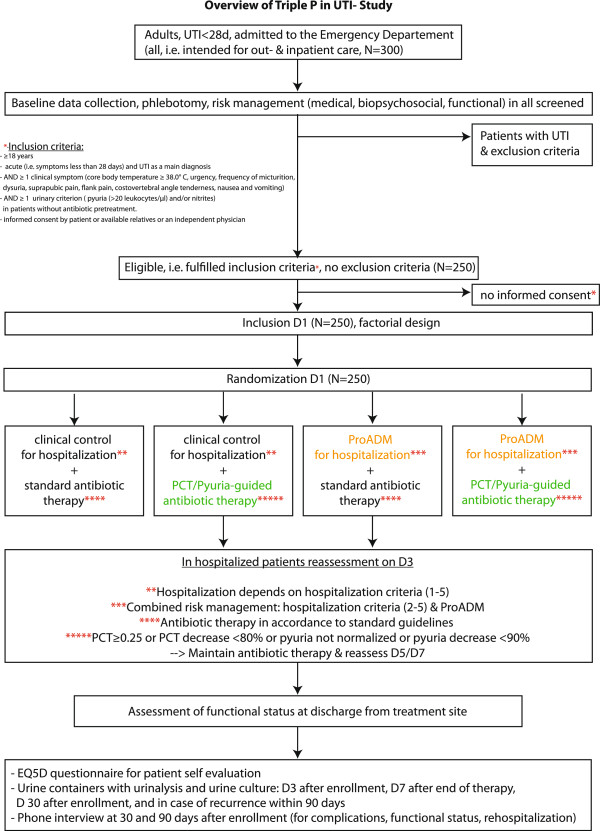
Urinary tract infections (UTIs) are among the most common infectious diseases and drivers of antibiotic use and in-hospital days. A reduction of antibiotic use potentially lowers the risk of antibiotic resistance. An early and adequate risk assessment combining medical, biopsychosocial and functional risk scores has the potential to optimize site-of-care decisions and thus allocation of limited health-care resources. The aim of this factorial design study is twofold: first, for Intervention A, it investigates antibiotic exposure of patients treated with a protocol based on the type of UTI, procalcitonin (PCT) and pyuria. Second, for Intervention B, it investigates the usefulness of the prognostic biomarker proadrenomedullin (ProADM) integrated into an interdisciplinary assessment bundle for site-of-care decisions.
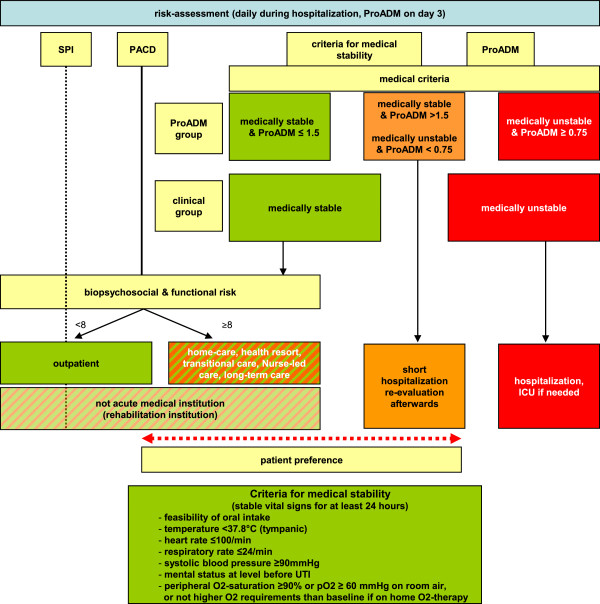
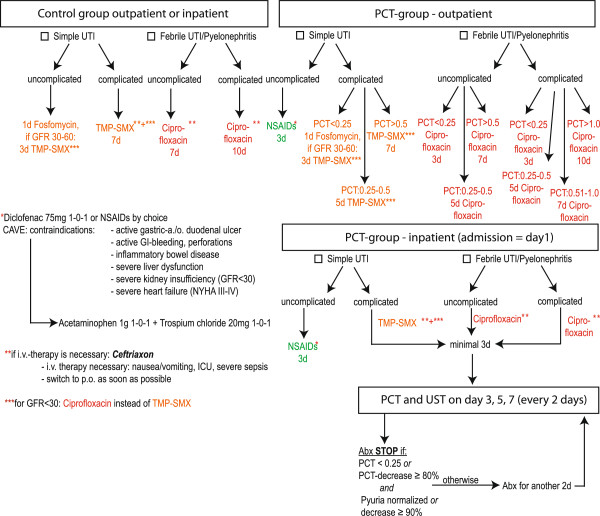
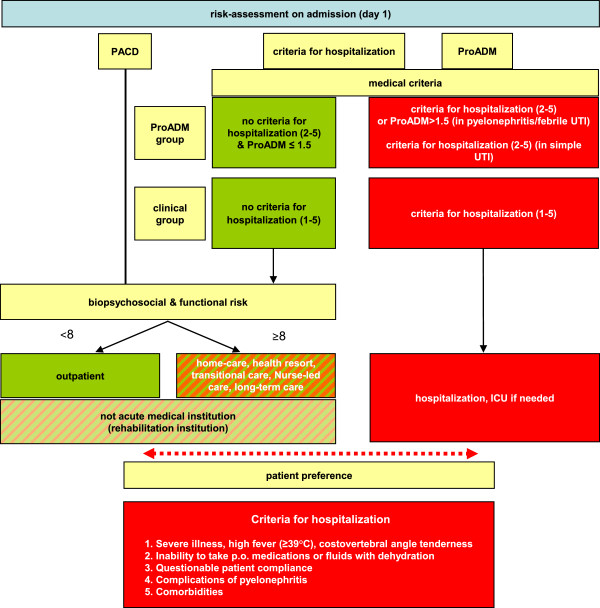
This randomized controlled open-label trial has a factorial design (2 × 2). Randomization of patients will be based on a pre-specified computer-generated randomization list and independent for the two interventions. Adults with UTI presenting to the emergency department (ED) will be screened and enrolled after providing informed consent. For our first Intervention (A), we developed a protocol based on previous observational research to recommend initiation and duration of antibiotic use based on the clinical presentation of UTI, pyuria and PCT levels. For our second intervention (B), an algorithm was developed to support site-of care decisions based on the prognostic marker ProADM and distinct nursing factors on days 1 and 3. Both interventions will be compared with a control group conforming to the guidelines. The primary endpoints for the two interventions will be: (A) overall exposure to antibiotics and (B) length of physician-led hospitalization within a follow-up of 30 days. Endpoints are assessed at discharge from hospital, and 30 and 90 days after admission. We plan to screen 300 patients and enroll 250 for an anticipated estimated loss of follow-up of 20%. This will provide adequate power for the two interventions.
This trial investigates two strategies for improved individualized medical care in patients with UTI. The minimally effective duration of antibiotic therapy is not known for UTIs, which is important for reducing the selection pressure for antibiotic resistance, costs and drug-related side effects. Triage decisions must be improved to reflect the true medical, biopsychosocial and functional risks in order to allocate patients to the most appropriate care setting and reduce hospital-acquired disability.
ISRCTN13663741.
尿路感染 (UTI) 是最常见的传染病之一,也是抗生素使用和住院天数的主要驱动因素。减少抗生素的使用可能会降低抗生素耐药的风险。结合医疗、生物心理社会和功能风险评分的早期和充分的风险评估有可能优化治疗场所的决策,并因此优化有限的卫生保健资源的分配。本因子设计研究的目的有两个:首先,对于干预措施 A,研究根据 UTI 类型、降钙素原 (PCT) 和脓尿制定的方案治疗的患者的抗生素暴露情况。其次,对于干预措施 B,研究预后生物标志物前肾上腺髓质素 (ProADM) 整合到跨学科评估包中用于治疗场所决策的有用性。
这是一项随机对照开放标签试验,采用因子设计(2×2)。患者的随机分组将基于预先指定的计算机生成的随机分组列表,并独立于两种干预措施。出现 UTI 的急诊科 (ED) 成年患者在提供知情同意后将进行筛选和入组。对于我们的第一项干预措施 (A),我们基于先前的观察性研究制定了一项方案,根据 UTI 的临床表现、脓尿和 PCT 水平推荐抗生素的起始和持续时间。对于我们的第二项干预措施 (B),开发了一种算法来支持基于预后标志物 ProADM 和第 1 天和第 3 天的不同护理因素的治疗场所决策。这两种干预措施都将与符合指南的对照组进行比较。这两种干预措施的主要终点是:(A) 抗生素总体暴露率和 (B) 医生主导的住院时间,随访时间为 30 天。终点在出院时以及入院后 30 天和 90 天进行评估。我们计划筛选 300 名患者,并招募 250 名患者,预计随访损失率为 20%。这将为两项干预措施提供足够的效力。
本试验研究了两种策略,以改善尿路感染患者的个体化医疗护理。对于 UTI,抗生素治疗的最小有效持续时间尚不清楚,这对于降低抗生素耐药性的选择压力、成本和药物相关副作用很重要。分诊决策必须改进,以反映真正的医疗、生物心理社会和功能风险,以便将患者分配到最合适的治疗场所,并减少医院获得性残疾。
ISRCTN81252622。