Department of Infectious Diseases, Leiden University Medical Center, PO, Box 9600, 2300 RC, Leiden, the Netherlands.
Department of Internal Medicine, Haga Hospital, The Hague, The Netherlands.
BMC Infect Dis. 2019 Feb 14;19(1):161. doi: 10.1186/s12879-019-3789-6.
A reduction in duration of antibiotic therapy is crucial in minimizing the development of antimicrobial resistance, drug-related side effects and health care costs. The minimal effective duration of antimicrobial therapy for febrile urinary tract infections (fUTI) remains a topic of uncertainty, especially in male patients, those of older age or with comorbidities. Biomarkers have the potential to objectively identify the optimal moment for cessation of therapy.
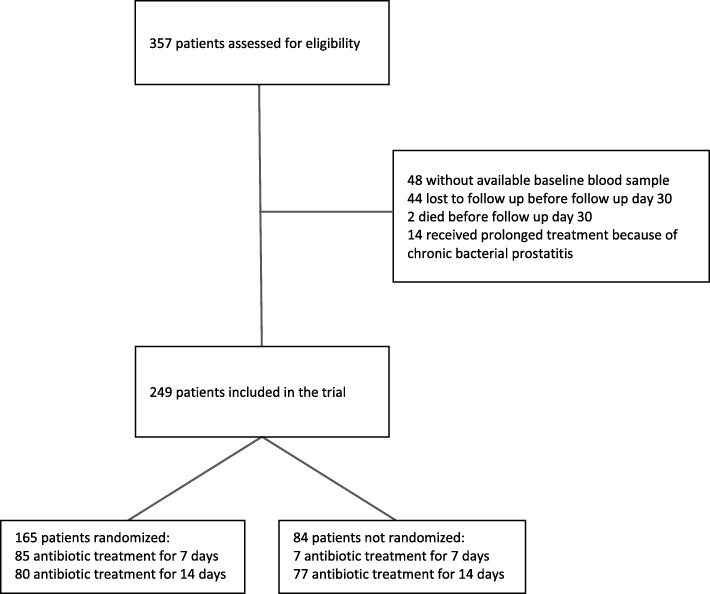
A secondary analysis of a randomized placebo-controlled trial among 35 primary care centers and 7 emergency departments of regional hospitals in the Netherlands. Women and men aged ≥18 years with a diagnosis of fUTI were randomly assigned to receive antibiotic treatment for 7 or 14 days. Patients indicated to receive antimicrobial treatment for more than 14 days were excluded from randomization. The biomarkers procalcitonin (PCT), mid-regional proadrenomedullin (MR-proADM), and C-reactive protein (CRP) were compared in their ability to predict clinical cure or failure through the 10-18 day post-treatment visit.
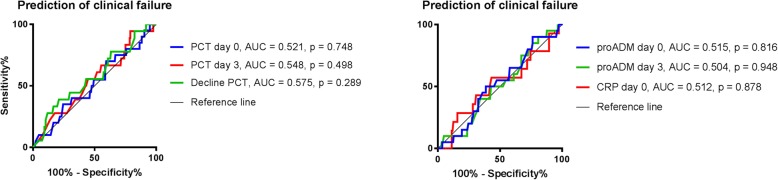
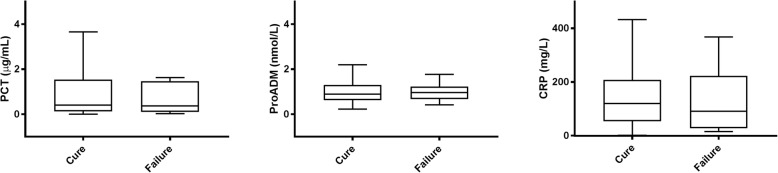
Biomarker concentrations were measured in 249 patients, with a clinical cure rate of 94% in the 165 randomized and 88% in the 84 non-randomized patients. PCT, MR-proADM and CRP concentrations did not differ between patients with clinical cure and treatment failure, and did not predict treatment outcome, irrespective of 7 or 14 day treatment duration (ROC 0.521; 0.515; 0.512, respectively). PCT concentrations at presentation were positively correlated with bacteraemia (τ = 0.33, p < 0.001) and presence of shaking chills (τ = 0.25, p < 0.001), and MR-proADM levels with length of hospital stay (τ = 0.40, p < 0.001), bacteraemia (τ = 0.33, p < 0.001), initial intravenous treatment (τ = 0.22, p < 0.001) and time to defervescence (τ = 0.21, p < 0.001). CRP did not display any correlation to relevant clinical parameters.
Although the biomarkers PCT and MR-proADM were correlated to clinical parameters indicating disease severity, they did not predict treatment outcome in patients with community acquired febrile urinary tract infection who were treated for either 7 or 14 days. CRP had no added value in the management of patients with fUTI.
The study was registered at ClinicalTrials.gov [ NCT00809913 ; December 16, 2008] and trialregister.nl [ NTR1583 ; December 19, 2008].
缩短抗生素治疗时间对于最大限度减少抗菌药物耐药性的发展、药物相关副作用和医疗保健成本至关重要。发热性尿路感染(fUTI)的最低有效抗生素治疗时间仍然是一个不确定的话题,尤其是在男性患者、老年患者或合并症患者中。生物标志物有可能客观地确定停止治疗的最佳时机。
对荷兰 35 个初级保健中心和 7 个地区医院急诊科进行的一项随机安慰剂对照试验的二次分析。≥18 岁的患有 fUTI 的女性和男性被随机分配接受 7 或 14 天的抗生素治疗。预计需要治疗超过 14 天的患者被排除在随机分组之外。通过治疗后 10-18 天的就诊,比较降钙素原(PCT)、中区域前肾上腺髓质素(MR-proADM)和 C 反应蛋白(CRP)在预测临床治愈或失败方面的能力。
在 249 名患者中测量了生物标志物浓度,随机分组的 165 名患者中有 94%的临床治愈率,非随机分组的 84 名患者中有 88%的临床治愈率。PCT、MR-proADM 和 CRP 浓度在临床治愈和治疗失败的患者之间没有差异,并且无论治疗持续时间为 7 天还是 14 天,都不能预测治疗结果(ROC 0.521;0.515;0.512)。就诊时的 PCT 浓度与菌血症呈正相关(τ=0.33,p<0.001)和寒战(τ=0.25,p<0.001)有关,MR-proADM 水平与住院时间(τ=0.40,p<0.001)、菌血症(τ=0.33,p<0.001)、初始静脉治疗(τ=0.22,p<0.001)和退热时间(τ=0.21,p<0.001)有关。CRP 与相关临床参数没有任何相关性。
尽管 PCT 和 MR-proADM 等生物标志物与表明疾病严重程度的临床参数相关,但它们不能预测接受 7 或 14 天治疗的社区获得性发热性尿路感染患者的治疗结果。CRP 对 fUTI 患者的管理没有额外价值。
该研究在 ClinicalTrials.gov 注册[ NCT00809913 ;2008 年 12 月 16 日]和 trialregister.nl [ NTR1583 ;2008 年 12 月 19 日]。