Aix-Marseille University, AP-HM, Service de Neuro-Oncologie, CHU Timone, 264 Rue Saint Pierre, 13005, Marseille, France.
Curr Neurol Neurosci Rep. 2013 May;13(5):347. doi: 10.1007/s11910-013-0347-2.
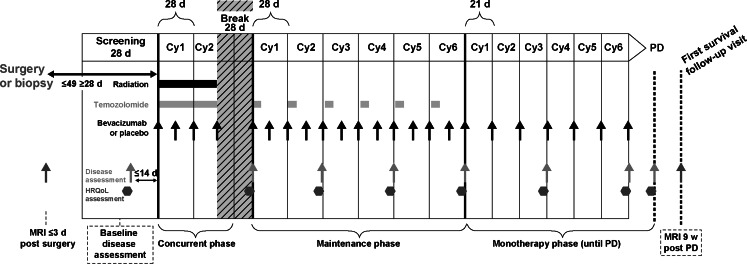
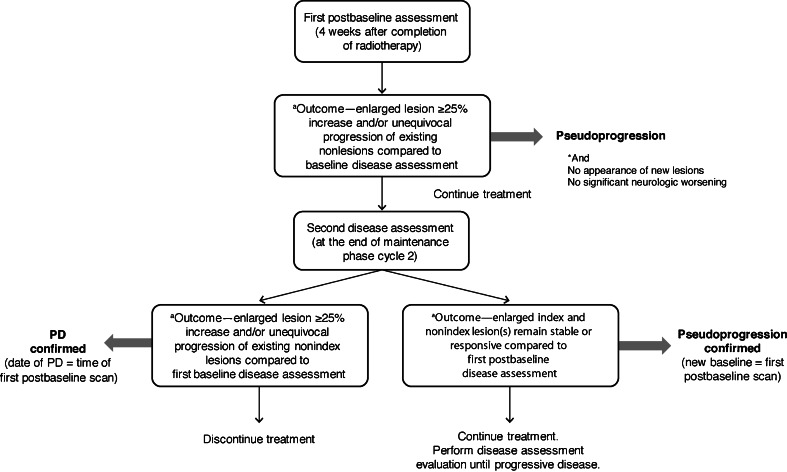
Since 1990, the primary criteria used for assessing response to therapy in high-grade gliomas were those developed by Macdonald and colleagues, which incorporated 2-dimensional area measurements of contrast-enhancing tumor regions, corticosteroid dosing, and clinical assessment to arrive at a designation of response, stable disease, or progression. Recent advances in imaging technology and targeted therapeutics, however, have exposed limitations of the Macdonald criteria and have highlighted the need for reevaluation of response assessment criteria. In 2010, the Response Assessment in Neuro-Oncology (RANO) Working Group published updated criteria to address this need and to standardize response assessment for high-grade gliomas. In 2009, prior to the publication of the RANO criteria, the randomized, placebo-controlled, multicenter, phase 3 AVAglio trial was designed and initiated to investigate the effectiveness of radiotherapy and temozolomide with or without bevacizumab in newly diagnosed glioblastoma. The AVAglio protocol enacted specific measures to adapt the Macdonald criteria to the frontline treatment setting and to antiangiogenic agent evaluation, including the incorporation of a T2/fluid-attenuated inversion recovery component, qualitative assessment of irregularly shaped contrast-enhancing lesions, and a decision tree for confirming or ruling out pseudoprogression. Moreover, the protocol outlines practical means by which these adapted response criteria can be implemented in the clinic. This article describes the evolution of radiographic response criteria for high-grade gliomas and highlights the similarities and differences between those implemented in the AVAglio study and those subsequently published by RANO.
自 1990 年以来,用于评估高级别神经胶质瘤治疗反应的主要标准是由 MacDonald 及其同事制定的,该标准纳入了对比增强肿瘤区域的二维面积测量、皮质类固醇剂量和临床评估,以确定反应、稳定疾病或进展的分类。然而,成像技术和靶向治疗的最新进展暴露了 MacDonald 标准的局限性,并强调需要重新评估反应评估标准。2010 年,神经肿瘤学反应评估(RANO)工作组发布了更新的标准来满足这一需求,并标准化高级别神经胶质瘤的反应评估。2009 年,在 RANO 标准发布之前,设计并启动了一项随机、安慰剂对照、多中心、3 期 AVAglio 试验,以研究放疗和替莫唑胺联合或不联合贝伐单抗在新诊断的胶质母细胞瘤中的疗效。AVAglio 方案采取了具体措施,使 MacDonald 标准适应一线治疗环境和抗血管生成药物评估,包括纳入 T2/液体衰减反转恢复成分、对不规则形状对比增强病变的定性评估,以及用于确认或排除假性进展的决策树。此外,该方案概述了在临床中实施这些适应反应标准的实用方法。本文描述了高级别神经胶质瘤的放射学反应标准的演变,并强调了在 AVAglio 研究中实施的标准与 RANO 随后发布的标准之间的相似点和不同点。