Severe Aplastic Anemia Studying Program, State Key Laboratory of Experimental Hematology, Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Science & Peking Union Medical College, Tianjin, PR China.
PLoS One. 2013;8(3):e56648. doi: 10.1371/journal.pone.0056648. Epub 2013 Mar 15.
Previous reports showed that outcome of rabbit antithymocyte globulin (rATG) was not satisfactory as the first-line therapy for severe aplastic anemia (SAA). We explored a modifying schedule of administration of rATG.
Outcomes of a cohort of 175 SAA patients, including 51 patients administered with standard protocol (3.55 mg/kg/d for 5 days) and 124 cases with optimized protocol (1.97 mg/kg/d for 9 days) of rATG plus cyclosporine (CSA), were analyzed retrospectively.
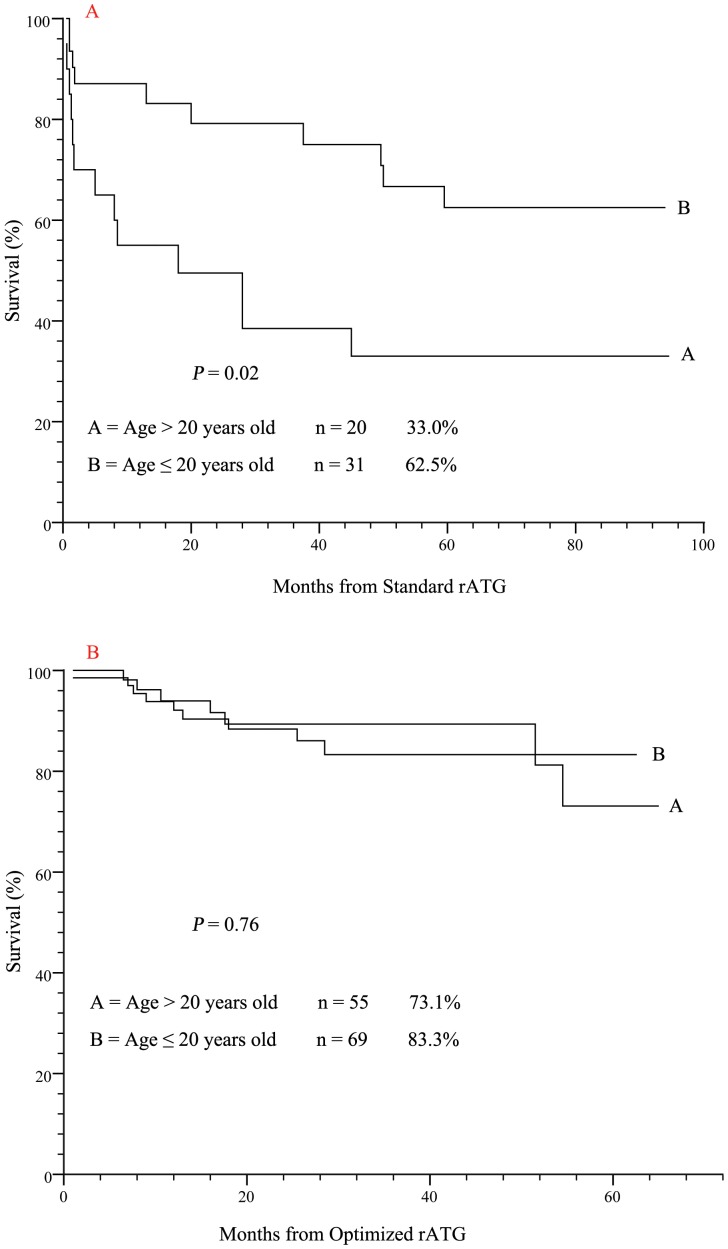
Of all 175 patients, response rates at 3 and 6 months were 36.6% and 56.0%, respectively. 51 cases received standard protocol had poor responses at 3 (25.5%) and 6 months (41.2%). However, 124 patients received optimized protocol had better responses at 3 (41.1%, P = 0.14) and 6 (62.1%, P = 0.01). Higher incidences of infection (57.1% versus 37.9%, P = 0.02) and early mortality (17.9% versus 0.8%, P<0.001) occurred in patients received standard protocol compared with optimized protocol. The 5-year overall survival in favor of the optimized over standard rATG protocol (76.0% versus. 50.3%, P<0.001) was observed. By multivariate analysis, optimized protocol (RR = 2.21, P = 0.04), response at 3 months (RR = 10.31, P = 0.03) and shorter interval (<23 days) between diagnosis and initial dose of rATG (RR = 5.35, P = 0.002) were independent favorable predictors of overall survival.
Optimized instead of standard rATG protocol in combination with CSA remained efficacious as a first-line immunosuppressive regimen for SAA.
先前的报告表明,兔抗胸腺细胞球蛋白(rATG)作为重型再生障碍性贫血(SAA)的一线治疗效果并不令人满意。我们探索了 rATG 给药方案的改良方案。
回顾性分析了 175 例 SAA 患者的队列结果,其中 51 例患者接受标准方案(3.55mg/kg/d,共 5 天),124 例患者接受 rATG 联合环孢素(CSA)的优化方案(1.97mg/kg/d,共 9 天)。
所有 175 例患者中,3 个月和 6 个月的反应率分别为 36.6%和 56.0%。51 例接受标准方案的患者在 3 个月(25.5%)和 6 个月(41.2%)时反应较差。然而,124 例接受优化方案的患者在 3 个月(41.1%,P=0.14)和 6 个月(62.1%,P=0.01)时反应更好。与优化方案相比,接受标准方案的患者感染发生率(57.1%比 37.9%,P=0.02)和早期死亡率(17.9%比 0.8%,P<0.001)更高。观察到优化 rATG 方案优于标准 rATG 方案的 5 年总生存率(76.0%比 50.3%,P<0.001)。多因素分析显示,优化方案(RR=2.21,P=0.04)、3 个月时的反应(RR=10.31,P=0.03)和 rATG 初始剂量诊断间隔较短(<23 天)(RR=5.35,P=0.002)是总生存率的独立有利预测因素。
与 CSA 联合使用优化而非标准 rATG 方案仍然是治疗 SAA 的有效一线免疫抑制方案。