State Key Laboratory of Experimental Hematology, National Clinical Research Center for Blood Diseases, Haihe Laboratory of Cell Ecosystem, Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Tianjin, China.
Department of Hematology, The Affiliated Yantai Yuhuangding Hospital of Qingdao University, Yantai, China.
Front Immunol. 2022 Feb 1;13:837335. doi: 10.3389/fimmu.2022.837335. eCollection 2022.
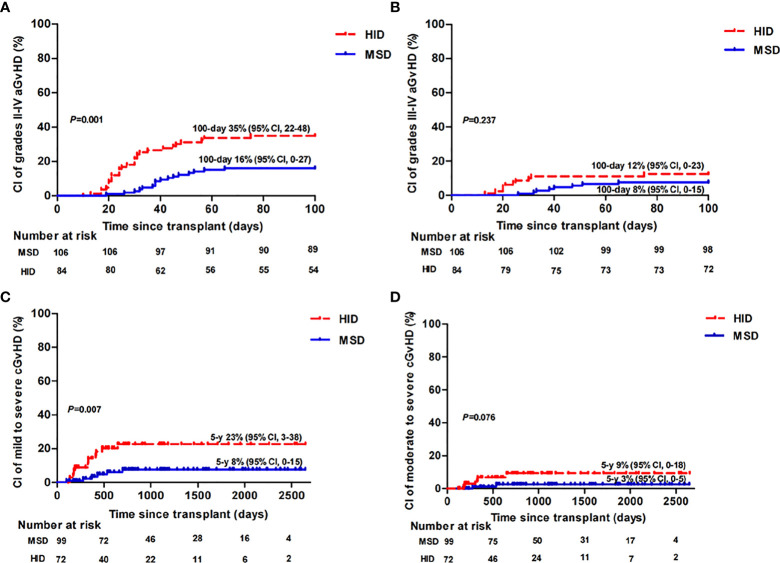
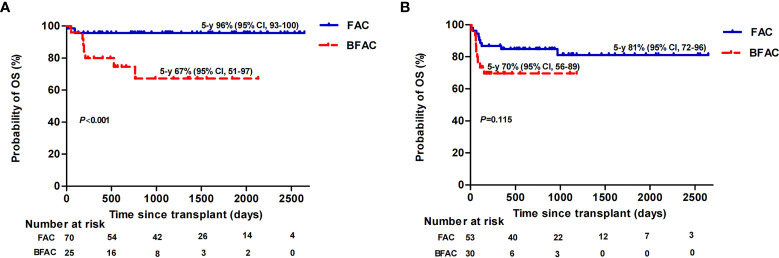
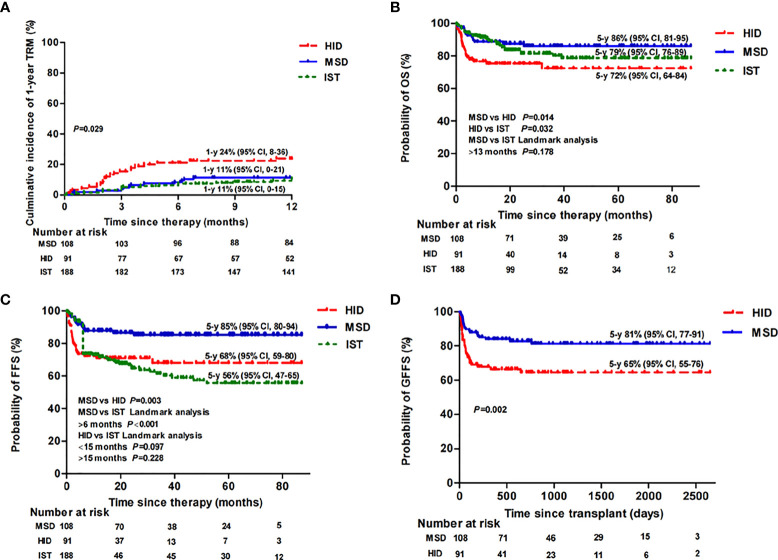
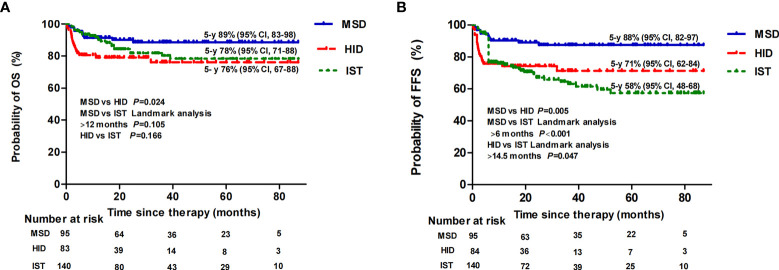
We retrospectively compared the outcomes of 387 consecutive patients with acquired aplastic anemia (AA) who underwent hematopoietic stem cell transplantation (HSCT) with a fludarabine-based conditioning regimen from matched sibling donors (MSD) (n = 108) or haploidentical donors (HID) (n = 91) and immunosuppressive therapy (IST) (n = 188) from 2014 to 2020 at our hospital. Compared with HID-HSCT, MSD-HSCT had a lower incidence of graft failure (1% 7%, = 0.062), grade II-IV acute graft versus host disease (aGvHD) (16% vs. 35%, = 0.001), and mild to severe chronic GvHD (cGvHD) (8% vs. 23%, = 0.007), but an equivalent incidence of grade III-IV aGvHD (8% vs. 12%, = 0.237) and moderate to severe cGvHD (3% vs. 9%, = 0.076). HSCT had superior blood count recovery at 3, 6, and 12 months compared with IST ( < 0.001). The estimated 5-year overall survival (OS) of the MSD, HID, and IST groups were 86%, 72%, and 79% ( = 0.02), respectively; accordingly, the failure-free survival (FFS) rates were 85%, 68%, and 56%, respectively ( < 0.001). For patients aged ≤40 years, the OS rate was still significantly superior for MSD-HSCT receipients compared to HID-HSCT receipients (89% vs. 76%, = 0.024) while the HID-HSCT recipients showed similar OS (76% vs. 78%, = 0.166) but superior FFS ( = 0.047) when follow-up was longer than 14.5 months in contrast to IST. In a multivariate analysis, HID-HSCT and a conditioning regimen that included busulfan were adversely related to OS among patients who received allografts. In conclusion, MSD-HSCT was the frontline choice for patients with severe AA aged ≤40 years, while HID-HSCT was as effective as IST for patients without an MSD.
我们回顾性比较了 2014 年至 2020 年期间,在我院接受亲缘相合供者(MSD)(n=108)或单倍体相合供者(HID)(n=91)基于氟达拉滨的预处理方案和免疫抑制治疗(IST)(n=188)造血干细胞移植(HSCT)的 387 例获得性再生障碍性贫血(AA)患者的结局。与 HID-HSCT 相比,MSD-HSCT 移植物失败发生率较低(1%比 7%,=0.062),Ⅱ-Ⅳ级急性移植物抗宿主病(aGvHD)(16%比 35%,=0.001)和轻-重度慢性移植物抗宿主病(cGvHD)(8%比 23%,=0.007)较低,但 Ⅲ-Ⅳ级 aGvHD 发生率相当(8%比 12%,=0.237)和中-重度 cGvHD(3%比 9%,=0.076)。HSCT 在 3、6 和 12 个月时的血液计数恢复优于 IST(<0.001)。MSD、HID 和 IST 组的 5 年总生存率(OS)分别为 86%、72%和 79%(=0.02),相应的无失败生存率(FFS)分别为 85%、68%和 56%(<0.001)。对于年龄≤40 岁的患者,MSD-HSCT 受体的 OS 率仍明显优于 HID-HSCT 受体(89%比 76%,=0.024),而 HID-HSCT 受体在随访时间超过 14.5 个月时,OS 相似(76%比 78%,=0.166)但 FFS 更好(=0.047)。在多变量分析中,HID-HSCT 和包含白消安的预处理方案与接受同种异体移植物的患者的 OS 不良相关。总之,对于年龄≤40 岁的严重 AA 患者,MSD-HSCT 是一线选择,而对于没有 MSD 的患者,HID-HSCT 与 IST 同样有效。