Agrawal Abhishek, Golovoy David, Nimjee Shahid, Ferrell Andrew, Smith Tony, Britz Gavin
Department of Radiology and Surgery, Division of Neurosurgery, Duke University Medical Center, Durham, North Carolina, USA.
Asian J Neurosurg. 2012 Oct;7(4):166-70. doi: 10.4103/1793-5482.106647.
Mechanical thrombectomy devices are gaining popularity in large vessel occlusions where chemical thrombolysis is usually futile. MERCI, Multi-MERCI, Penumbra and SWIFT trails have elevated the status of mechanical thrombectomy from being a complementary treatment modality to mainstream stroke intervention. The aim of this study was to compare our immediate recanalization rates with available mechanical devices.
A retrospective review from March 2009 to August 2012 was performed on patients who underwent mechanical thrombectomy for large vessel occlusion. Cases where IATPA and/or balloon angioplasty was performed without mechanical thrombectomy were excluded from the study. Recanalization rates were assessed immediately post-procedure by follow-up angiography. TICI scores were used to quantify the extent of recanalization and the residual clot burden.
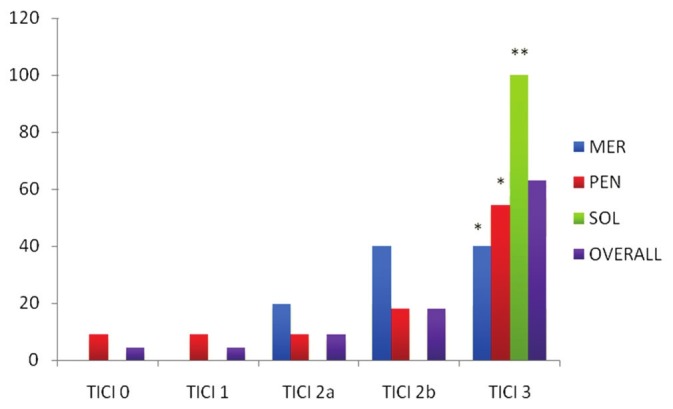
Twenty two procedures were performed on 20 patients using Merci (MER):5; Penumbra (PEN):11; Solitaire-FR (SOL):6. Two patients underwent intervention using both Merci and Penumbra devices. The M:F ratio was 1.2:1. The most common vascular territory involved was the right MCA (9/20) followed by left MCA (5/20), left ICA (2/20), basilar (3/20) and vertebral arteries (1/20). The average door to needle time was 210 minutes [MER: 184.4; PEN: 249.2; SOL: 162]. Additional procedures were performed in 63.4% (14/22) of the patients [MER: 80% (4/5); PEN: 72.7% (8/11) and SOL: 33.3% (2/6)]. Vasospasm was observed in MER: 20% (1/5); PEN: 9.1% (1/11); SOL: 0% (0/6)]. Complete recanalization was achieved in 59.1% (13/22) [MER: 40% (2/5); PEN: 45.5% (5/11); SOL: 100% (6/6)]. The rate of complete recanalization was statistically significant for the Solitaire group vs. the MERCI group (P=0.0062) as well as the Penumbra group (0.0025). The average pre-procedure TICI was 0.4 [MER: 0.6; PEN: 0.3; SOL: 0.3], while the average post-procedure TICI was 2.5 [MER: 2.4; PEN: 2.3; SOL: 3.0].
The study reveals a higher rate of angiographic recanalization using the Solitaire-FR device, requiring a lesser number of passes and other associated procedures as compared to MERCI and Penumbra. Thus, Stentrievers (Solitaire-FR) are advantageous in faster device delivery and quick flow restoration. However, future prospective randomized large trials are required to confirm these early results.
在大血管闭塞性疾病中,机械取栓装置正越来越受欢迎,而化学溶栓通常效果不佳。MERCI、Multi - MERCI、Penumbra和SWIFT试验已将机械取栓的地位从一种辅助治疗方式提升为主流的卒中干预手段。本研究的目的是将我们的即时再通率与现有的机械装置进行比较。
对2009年3月至2012年8月期间因大血管闭塞接受机械取栓的患者进行回顾性研究。未进行机械取栓而仅行IATPA和/或球囊血管成形术的病例被排除在研究之外。术后立即通过随访血管造影评估再通率。使用TICI评分来量化再通程度和残余血栓负荷。
对20例患者进行了22次手术,使用Merci(MER):5例;Penumbra(PEN):11例;Solitaire - FR(SOL):6例。2例患者同时使用Merci和Penumbra装置进行了干预。男女比例为1.2:1。最常受累的血管区域是右侧大脑中动脉(9/20),其次是左侧大脑中动脉(5/20)、左侧颈内动脉(2/20)、基底动脉(3/20)和椎动脉(1/20)。平均从入院到穿刺时间为210分钟[MER:184.4;PEN:249.2;SOL:162]。63.4%(14/22)的患者进行了额外的手术[MER:80%(4/5);PEN:72.7%(8/11);SOL:33.3%(2/6)]。观察到血管痉挛的情况为:MER:20%(1/5);PEN:9.1%(1/11);SOL:0%(0/6)]。59.1%(13/22)实现了完全再通[MER:40%(2/5);PEN:45.5%(5/11);SOL:100%(6/6)]。Solitaire组与MERCI组(P = 0.0062)以及Penumbra组(0.0025)相比,完全再通率具有统计学意义。术前平均TICI为0.4[MER:0.6;PEN:0.3;SOL:0.3],而术后平均TICI为2.5[MER:2.4;PEN:2.3;SOL:3.0]。
该研究表明,与Merci和Penumbra相比,使用Solitaire - FR装置血管造影再通率更高,所需的操作次数和其他相关手术更少。因此,支架取栓器(Solitaire - FR)在更快的装置输送和快速血流恢复方面具有优势。然而,需要未来进行前瞻性随机大型试验来证实这些早期结果。