Department of Pharmacy and Pharmacology, University of Bath, Bath, United Kingdom.
PLoS One. 2013 Apr 4;8(4):e60247. doi: 10.1371/journal.pone.0060247. Print 2013.
Asthma is common during pregnancy, however research is limited regarding the extent and timing of changes in asthma management associated with pregnancy.
To determine the prevalence of asthma during pregnancy and identify changes in treatment and asthma exacerbation rates associated with pregnancy, while controlling for seasonal influences.
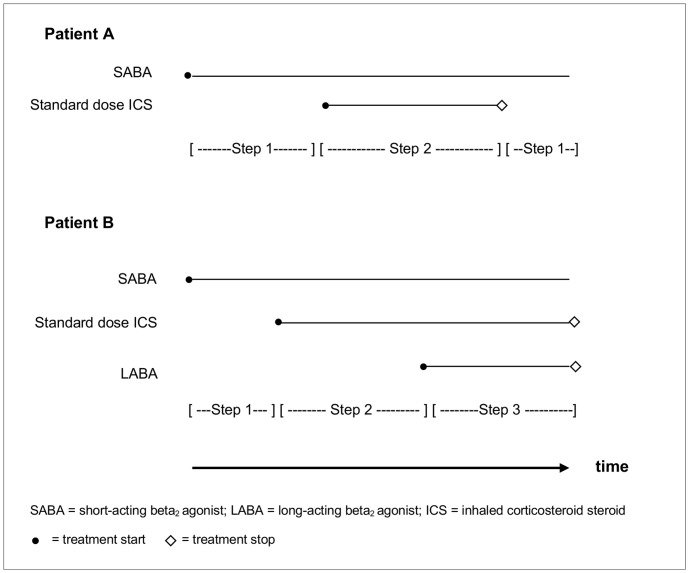
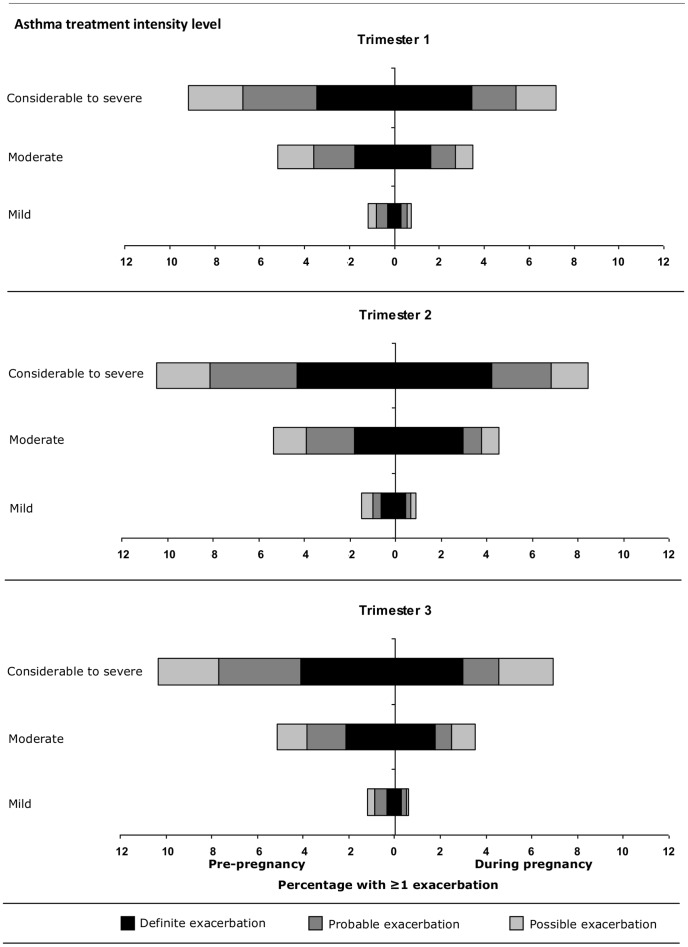
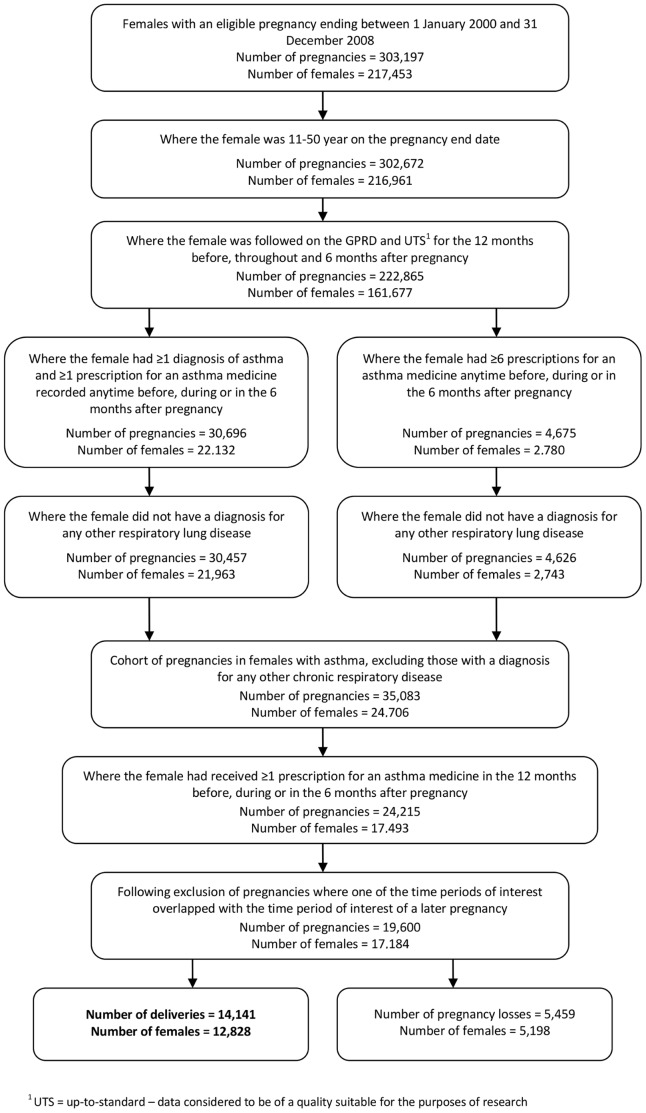
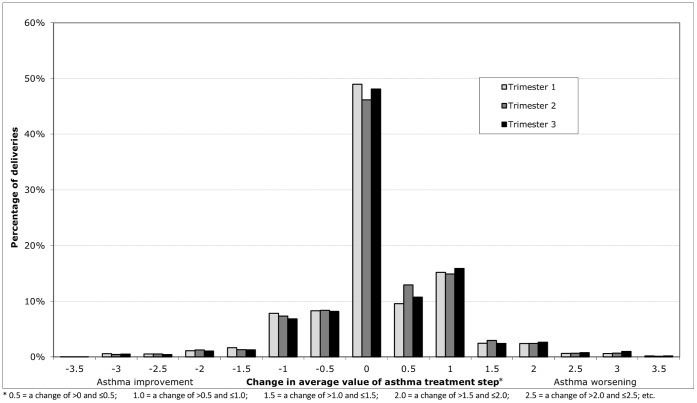
Pregnant women with asthma were identified from the UK General Practice Research Database between 2000 and 2008. For each woman asthma medication prescribed during the study period was identified; for each product combination the British Thoracic Society medication-defined asthma treatment step was identified. Asthma exacerbations were identified during pregnancy and in the corresponding 12 months prior. Analyses of changes in asthma treatment and exacerbation rates during pregnancy relative to the corresponding period 12 months prior, to control for seasonality, were stratified by trimester and asthma treatment intensity level.
The prevalence of treated asthma in pregnancies resulting in a delivery was 8.3%. From 14,141 pregnancies, in 12,828 women with asthma, 68.4% received prescriptions for a short-acting β2-agonist and 41.2% for inhaled corticosteroids; 76.5% were managed with asthma treatment Step 1 or 2. Poor persistence to inhaled corticosteroids, defined as a gap of up to 60 days between prescriptions, was common. In 45.0% of pregnancies, an increase in average treatment step was observed whereas in 25.6% the treatment step decreased. Treatment intensity remained the same in 29.5% of pregnancies. Exacerbations occurred in 4.8% of pregnancies compared to 5.9% in the same season the year before (p<0.001).
Exacerbation rates during pregnancy were slightly lower than in the year before. However, treatment patterns and exacerbation rates in this study suggest asthma control during pregnancy is variable, and women may require close monitoring especially in those with evidence of poor control before pregnancy.
哮喘在怀孕期间很常见,但关于与怀孕相关的哮喘管理的程度和时间变化的研究有限。
确定怀孕期间哮喘的患病率,并确定与怀孕相关的治疗变化和哮喘恶化率,同时控制季节性影响。
在 2000 年至 2008 年间,从英国全科医生研究数据库中确定患有哮喘的孕妇。在研究期间,为每位妇女开的哮喘药物进行鉴定;对于每个产品组合,确定英国胸科协会药物定义的哮喘治疗步骤。在怀孕期间和之前的 12 个月期间确定哮喘恶化情况。为了控制季节性,根据妊娠期间和之前的 12 个月的三阶段和哮喘治疗强度水平,分析哮喘治疗和恶化率的变化。
导致分娩的妊娠中治疗性哮喘的患病率为 8.3%。在 14141 次妊娠中,在 12828 名患有哮喘的妇女中,68.4%接受了短效β2-激动剂的处方,41.2%接受了吸入皮质类固醇的处方;76.5%的人接受了哮喘治疗第 1 或 2 步的治疗。常见的吸入皮质类固醇的持续使用不佳,定义为处方之间的差距长达 60 天。在 45.0%的妊娠中,观察到平均治疗步骤增加,而在 25.6%的妊娠中治疗步骤减少。29.5%的妊娠治疗强度保持不变。与前一年同期(p<0.001)相比,4.8%的妊娠中发生了恶化。
怀孕期间恶化率略低于前一年。然而,本研究中的治疗模式和恶化率表明,怀孕期间的哮喘控制情况各不相同,尤其是那些在怀孕前就存在控制不佳的证据的妇女,可能需要密切监测。