Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
Clin Mol Hepatol. 2013 Mar;19(1):29-35. doi: 10.3350/cmh.2013.19.1.29. Epub 2013 Mar 25.
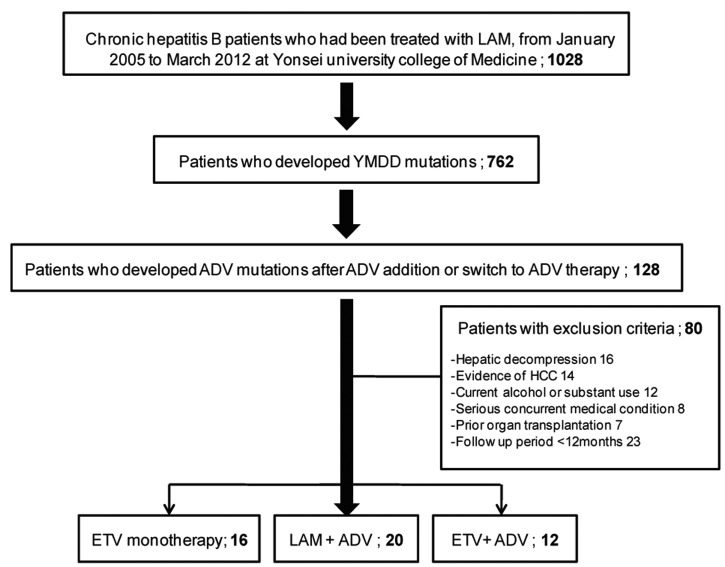
BACKGROUND/AIMS: The incidence of multidrug-resistant (MDR) chronic hepatitis B (CHB) during sequential lamivudine (LAM) and adefovir dipivoxil (ADV) treatment is increasing. We investigated the antiviral efficacies of various rescue regimens in patients who failed sequential LAM-ADV treatment.
Forty-eight patients (83.3% of whom were HBeAg-positive) who failed sequential LAM-ADV treatment were treated with one of the following regimens: entecavir (ETV) (1 mg) monotherapy (n=16), LAM+ADV combination therapy (n=20), or ETV (1 mg)+ADV combination therapy (n=12). All patients had confirmed genotypic resistance to both LAM and ADV and were evaluated every 12 weeks.
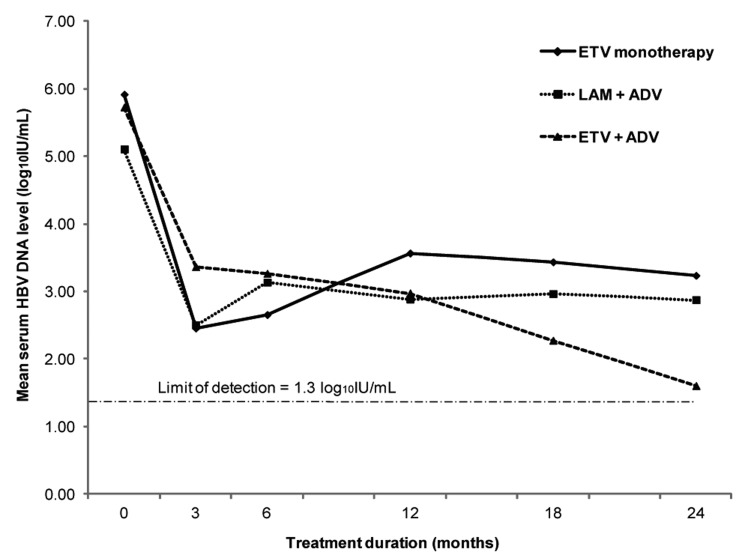
The baseline characteristics and treatment duration did not differ significantly among the study groups. During the treatment period (median duration: 100 weeks), the decline of serum HBV DNA from baseline tended to be greatest in the ETV+ADV group at all-time points (week 48: -2.55 log(10) IU/mL, week 96: -4.27 log(10) IU/mL), but the difference was not statistically significant. The ETV+ADV group also tended to have higher virologic response rates at 96 weeks compared to the ETV monotherapy or LAM+ADV groups (40.0% vs. 20.0% or 20.0%, P=0.656), and less virologic breakthrough was observed compared to the ETV monotherapy or LAM+ADV groups (8.3% vs. 37.5% or 30.0%; P=0.219), but again, the differences were not statistically significant. HBeAg loss occurred in one patient in the ETV+ADV group, in two in the ETV monotherapy group, and in none of the LAM+ADV group. The safety profiles were similar in each arm.
There was a nonsignificant tendency toward better antiviral efficacy with ETV+ADV combination therapy compared to LAM+ADV combination therapy and ETV monotherapy for MDR CHB in Korea, where tenofovir is not yet available.
背景/目的:序贯应用拉米夫定(LAM)和阿德福韦酯(ADV)治疗后,多重耐药(MDR)慢性乙型肝炎(CHB)的发生率正在增加。我们研究了在序贯 LAM-ADV 治疗失败的患者中,各种挽救方案的抗病毒疗效。
48 例(83.3%为 HBeAg 阳性)序贯 LAM-ADV 治疗失败的患者接受以下治疗方案之一:恩替卡韦(ETV)(1mg)单药治疗(n=16)、LAM+ADV 联合治疗(n=20)或 ETV(1mg)+ADV 联合治疗(n=12)。所有患者均对 LAM 和 ADV 均有明确的基因型耐药,并每 12 周进行一次评估。
研究组之间的基线特征和治疗持续时间无显著差异。在治疗期间(中位持续时间:100 周),所有时间点 ETV+ADV 组血清 HBV DNA 从基线下降幅度最大(第 48 周:-2.55 log10IU/mL,第 96 周:-4.27 log10IU/mL),但差异无统计学意义。与 ETV 单药治疗或 LAM+ADV 组相比,第 96 周时 ETV+ADV 组的病毒学应答率也较高(40.0%比 20.0%或 20.0%,P=0.656),并且与 ETV 单药治疗或 LAM+ADV 组相比,病毒学突破较少(8.3%比 37.5%或 30.0%;P=0.219),但差异无统计学意义。在 ETV+ADV 组中有 1 例患者发生 HBeAg 丢失,在 ETV 单药治疗组中有 2 例,在 LAM+ADV 组中无 1 例。各治疗组的安全性相似。
在韩国,由于尚未使用替诺福韦,与 LAM+ADV 联合治疗和 ETV 单药治疗相比,ETV+ADV 联合治疗对 MDR CHB 具有更好的抗病毒疗效,但差异无统计学意义。