Institute of Microbiology and Immunology, School of Life Sciences, National Yang-Ming University, Taipei, Taiwan.
PLoS One. 2013 Apr 17;8(4):e61448. doi: 10.1371/journal.pone.0061448. Print 2013.
Hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) is a major global health problem. A few risk calculators have been developed using mainly HBV seromarkers as predictors. However, serum HBV DNA level, HBV genotype, and mutants are not routinely checked in regular health examinations. This study aimed to assess the predictability of HCC risk in chronic hepatitis B patients, using a combination of liver-related seromarkers combined with or without HBV seromarkers.
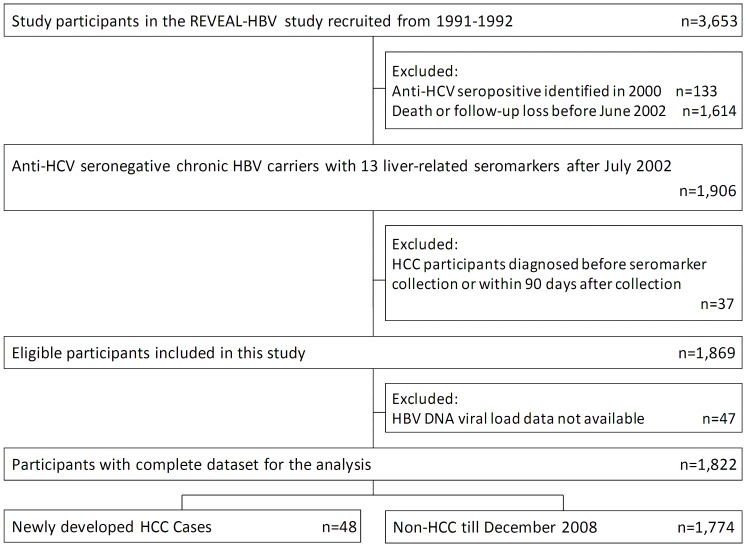
A prospective cohort of 1,822 anti-HCV-seronegative chronic HBV carriers was included in this study. Liver-related seromarkers including aspartate aminotransferase (AST), alanine aminotransferase (ALT), alpha-fetoprotein (AFP), gamma-glutamyltransferase (GGT), total bilirubin, total protein, albumin, serum globulins, apolipoprotein A1, and apolipoprotein B were examined. Hazard ratios of HCC with 95% confidence intervals were estimated using Cox proportional hazards regression models. Regression coefficients of seromarkers significantly associated with HCC risk in multivariate analyses were used to create integer risk scores. The predictability of various risk models were assessed by area under receiver operating characteristic curves (AUROCs).
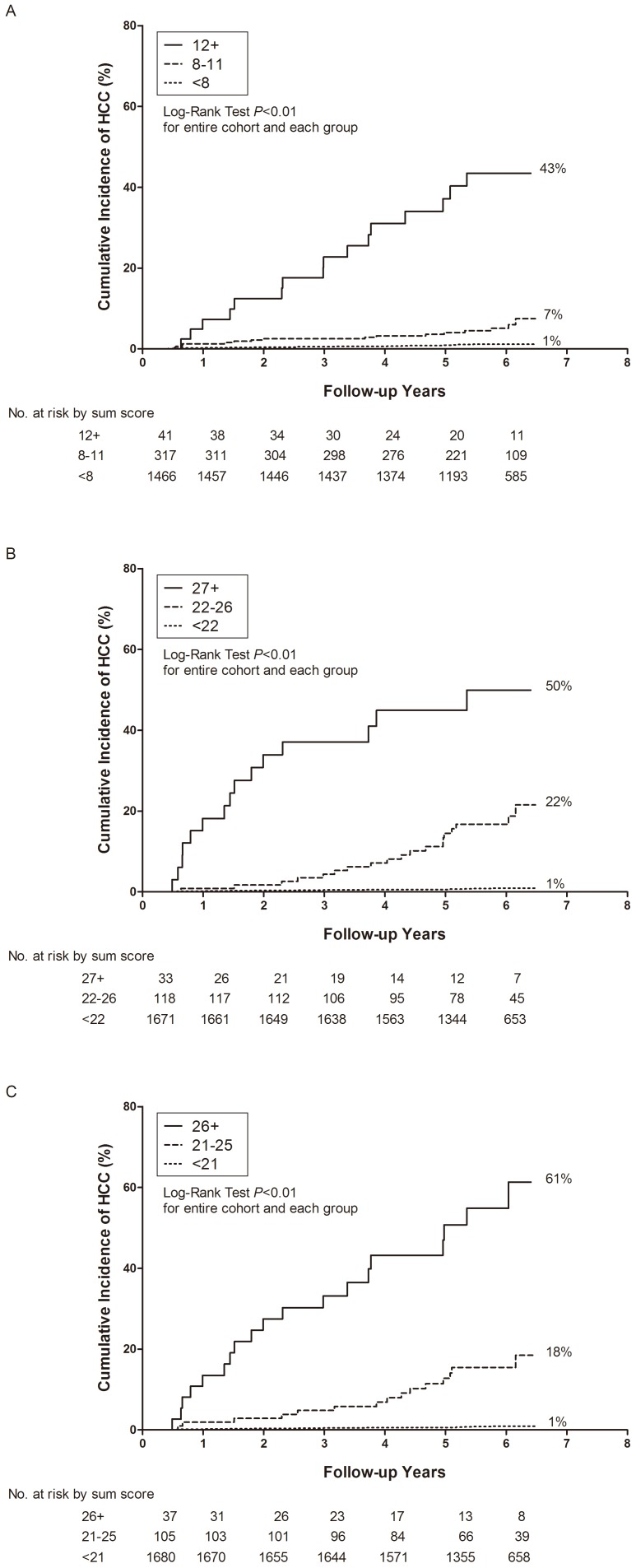
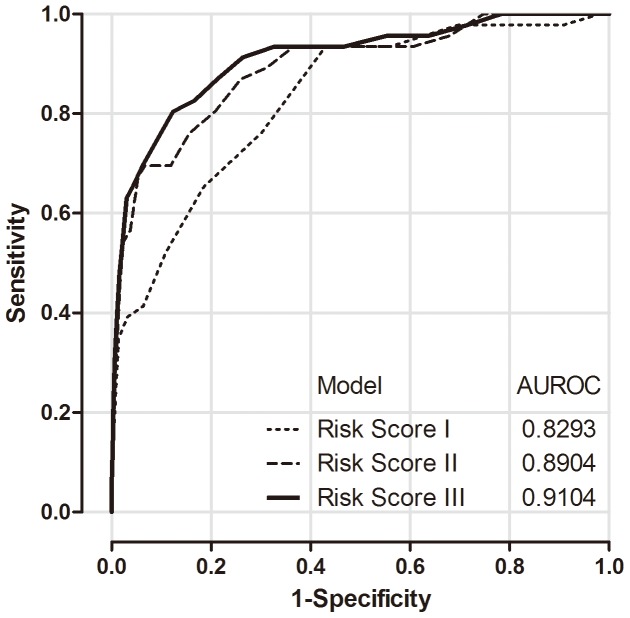
During a median follow-up of 5.9 years, 48 newly-developed HCC cases were ascertained. Elevated serum levels of ALT (≥ 28 U/L), AFP (≥ 5 ng/mL), and GGT (≥ 41 U/L), an increased AST/ALT ratio (AAR, ≥ 1), and lowered serum levels of albumin (≤ 4.1 g/dL) and alpha-1 globulin (≤ 0.2 g/dL) were significantly associated with an increased HCC risk (P<0.05) in multivariate analysis. The risk model incorporating age, gender, AAR, and serum levels of ALT, AFP, GGT, albumin, and alpha-1 globulin had an AUROC of 0.89 for predicting 6-year HCC incidence. The AUROC was 0.91 after the addition of HBV seromarkers into the model, and 0.83 for the model without liver-related seromarkers, with the exception of ALT.
Liver-related seromarkers may be combined into useful risk models for predicting HBV-related HCC risk.
乙型肝炎病毒(HBV)相关肝细胞癌(HCC)是一个全球性的主要健康问题。已经开发了一些风险计算器,主要使用 HBV 血清标志物作为预测因子。然而,在常规健康检查中,通常不检查血清 HBV DNA 水平、HBV 基因型和突变体。本研究旨在评估使用结合肝相关血清标志物与或不结合 HBV 血清标志物的方法,预测慢性乙型肝炎患者 HCC 风险的能力。
本研究纳入了前瞻性队列中 1822 名抗 HCV 阴性的慢性 HBV 携带者。检查了与肝脏相关的血清标志物,包括天门冬氨酸氨基转移酶(AST)、丙氨酸氨基转移酶(ALT)、甲胎蛋白(AFP)、γ-谷氨酰转移酶(GGT)、总胆红素、总蛋白、白蛋白、血清球蛋白、载脂蛋白 A1 和载脂蛋白 B。使用 Cox 比例风险回归模型估计 HCC 的风险比(HR)和 95%置信区间。在多变量分析中,与 HCC 风险显著相关的血清标志物的回归系数用于创建整数风险评分。通过接收者操作特征曲线下面积(AUROC)评估各种风险模型的预测能力。
在中位数为 5.9 年的随访期间,确定了 48 例新发生的 HCC 病例。在多变量分析中,血清 ALT(≥28 U/L)、AFP(≥5ng/mL)和 GGT(≥41 U/L)水平升高、AST/ALT 比值(AAR,≥1)升高以及血清白蛋白(≤4.1g/dL)和α-1 球蛋白(≤0.2g/dL)水平降低与 HCC 风险增加显著相关(P<0.05)。纳入年龄、性别、AAR 以及血清 ALT、AFP、GGT、白蛋白和α-1 球蛋白水平的风险模型,对预测 6 年 HCC 发生率的 AUROC 为 0.89。将 HBV 血清标志物添加到模型中后,AUROC 为 0.91,而不包括与肝脏相关的血清标志物(除了 ALT)的模型的 AUROC 为 0.83。
肝相关血清标志物可结合成有用的风险模型,用于预测 HBV 相关 HCC 风险。