Ohtaka Kazuto, Hida Yasuhiro, Kaga Kichizo, Kato Tatsuya, Muto Jun, Nakada-Kubota Reiko, Hirano Satoshi, Matsui Yoshiro
Department of Cardiovascular and Thoracic Surgery, Hokkaido University Graduate School of Medicine, Sapporo, Hokkaido, Japan.
J Cardiothorac Surg. 2013 Apr 24;8:111. doi: 10.1186/1749-8090-8-111.
Lung tumors showing ground-glass opacities on high-resolution computed tomography indicate the presence of inflammation, atypical adenomatous hyperplasia, or localized bronchioloalveolar carcinoma. We adopted a two-staged video-assisted thoracoscopic lobectomy strategy involving completion lobectomy for localized bronchioloalveolar carcinoma with an invasive component according to postoperative pathological examination by permanent section after partial resection.
Forty-one patients with undiagnosed small peripheral ground-glass opacity lesions underwent partial resection from 2001 to 2007 in Hokkaido University Hospital. Localized bronchioloalveolar carcinoma was classified according to the Noguchi classification for adenocarcinoma. Malignant lesions other than Noguchi types A and B were considered for completion lobectomy and systemic mediastinal lymphadenectomy. Perioperative data of completion video-assisted thoracoscopic lobectomies were compared with data of 67 upfront video-assisted thoracoscopic lobectomies for clinical stage IA adenocarcinoma performed during the same period.
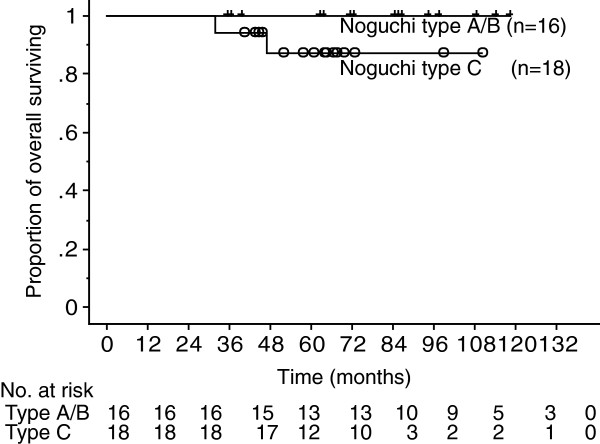
Postoperative pathological examination revealed 35 malignant and 6 non-malignant diseases. Histologically, all of the malignant diseases were adenocarcinomas of Noguchi type A (n = 7), B (n = 9), C (n = 18), and F (n = 1). Eleven of 19 patients (58%) with Noguchi type C or F underwent two-staged video-assisted thoracoscopic lobectomy. Three patients refused a second surgery. There was no cancer recurrence. The two-staged lobectomy group had a significantly longer operative time and more blood loss than the upfront lobectomy group. There was no surgical mortality or cancer recurrence.
Two-staged lobectomy for undiagnosed small peripheral ground-glass opacity lesions showed satisfactory oncological results. However, low compliance for and invasiveness of the second surgery are concerns associated with this strategy.
在高分辨率计算机断层扫描上显示磨玻璃影的肺部肿瘤提示存在炎症、非典型腺瘤样增生或局限性细支气管肺泡癌。我们采用了两阶段电视辅助胸腔镜肺叶切除术策略,即根据部分切除术后永久切片的术后病理检查结果,对具有浸润成分的局限性细支气管肺泡癌进行完整肺叶切除术。
2001年至2007年,北海道大学医院对41例未确诊的小的外周磨玻璃影病变患者进行了部分切除术。局限性细支气管肺泡癌根据腺癌的野口分类进行分类。除野口A和B型以外的恶性病变考虑行完整肺叶切除术和系统性纵隔淋巴结清扫术。将完整电视辅助胸腔镜肺叶切除术的围手术期数据与同期进行的67例临床IA期腺癌的一期电视辅助胸腔镜肺叶切除术的数据进行比较。
术后病理检查发现35例恶性疾病和6例非恶性疾病。组织学上,所有恶性疾病均为野口A型(n = 7)、B型(n = 9)、C型(n = 18)和F型(n = 1)腺癌。19例野口C型或F型患者中有11例(58%)接受了两阶段电视辅助胸腔镜肺叶切除术。3例患者拒绝二次手术。无癌症复发。两阶段肺叶切除术组的手术时间明显长于一期肺叶切除术组,失血量也更多。无手术死亡或癌症复发。
对于未确诊的小的外周磨玻璃影病变,两阶段肺叶切除术显示出令人满意的肿瘤学结果。然而,二次手术的低依从性和侵袭性是该策略相关的问题。