Department of Pathology, Memorial Sloan-Kettering Cancer Center, New York, NY, USA.
Mod Pathol. 2013 Oct;26(10):1307-19. doi: 10.1038/modpathol.2013.74. Epub 2013 Apr 26.
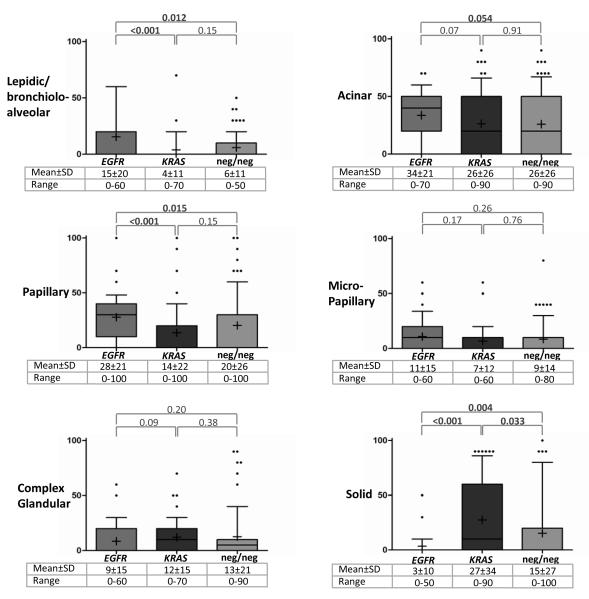
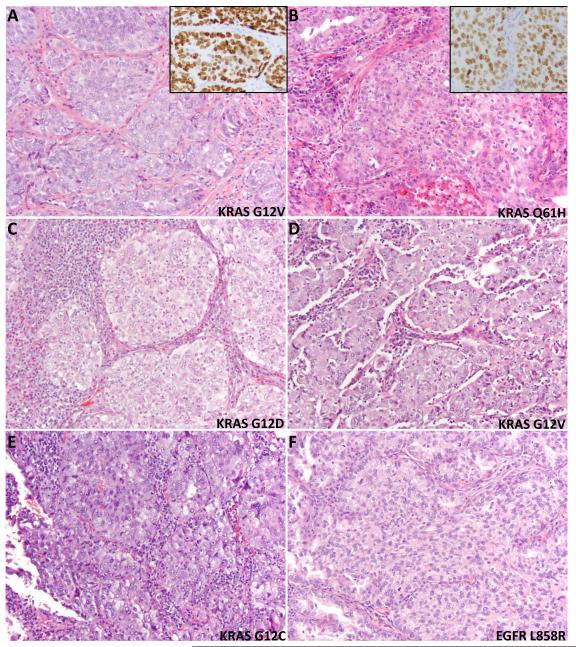
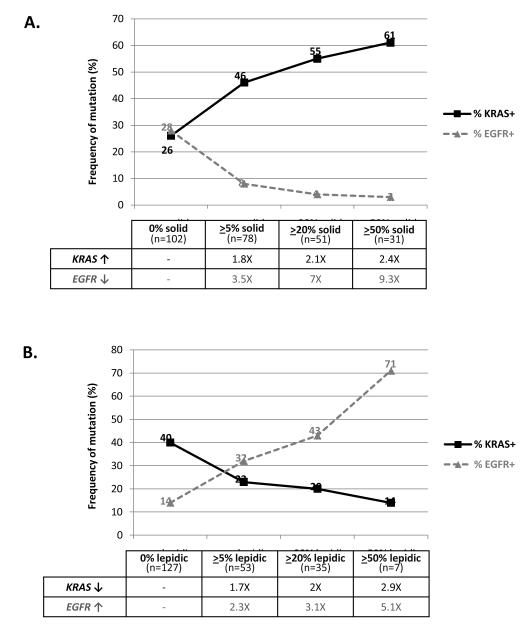
KRAS mutations define a clinically distinct subgroup of lung adenocarcinoma patients, characterized by smoking history, resistance to EGFR-targeted therapies, and adverse prognosis. Whether KRAS-mutated lung adenocarcinomas also have distinct histopathological features is not well established. We tested 180 resected lung adenocarcinomas for KRAS and EGFR mutations by high-sensitivity mass spectrometry-based genotyping (Sequenom) and PCR-based sizing assays. All tumors were assessed for the proportion of standard histological patterns (lepidic, acinar, papillary, micropapillary, solid, and mucinous), several other histological and clinical parameters, and TTF-1 expression by immunohistochemistry. Among 180 carcinomas, 63 (35%) had KRAS mutations (KRAS+), 35 (19%) had EGFR mutations (EGFR+), and 82 (46%) had neither mutation (KRAS-/EGFR-). Solid growth pattern was significantly over-represented in KRAS+ carcinomas: the mean±s.d. for the amount of solid pattern in KRAS+ carcinomas was 27±34% compared with 3±10% in EGFR+ (P<0.001) and 15±27% in KRAS-/EGFR- (P=0.033) tumors. Furthermore, at least focal (≥20%) solid component was more common in KRAS+ (28/63; 44%) compared with EGFR+ (2/35; 6%; P<0.001) and KRAS-/EGFR- (21/82; 26%; P=0.022) carcinomas. KRAS mutations were also over-represented in mucinous carcinomas and were significantly associated with the presence of tumor-infiltrating leukocytes and heavier smoking history. EGFR mutations were associated with non-mucinous non-solid patterns, particularly lepidic and papillary, lack of necrosis, lack of cytological atypia, hobnail cytology, TTF-1 expression, and never/light smoking history. In conclusion, extended molecular and clinicopathological analysis of lung adenocarcinomas reveals a novel association of KRAS mutations with solid histology and tumor-infiltrating inflammatory cells and expands on several previously recognized morphological and clinical associations of KRAS and EGFR mutations. Solid growth pattern was recently shown to be a strong predictor of aggressive behavior in lung adenocarcinomas, which may underlie the unfavorable prognosis associated with KRAS mutations in these tumors.
KRAS 突变定义了一组具有临床特征的肺腺癌患者,其特征为吸烟史、对 EGFR 靶向治疗的耐药性和不良预后。KRAS 突变的肺腺癌是否也具有独特的组织病理学特征尚不清楚。我们通过基于高灵敏度质谱的基因分型(Sequenom)和基于 PCR 的大小测定法检测了 180 例切除的肺腺癌中的 KRAS 和 EGFR 突变。所有肿瘤均评估了标准组织学模式(贴壁型、腺泡型、乳头状、微乳头状、实体型和黏液型)、其他几种组织学和临床参数以及 TTF-1 的免疫组织化学表达。在 180 例癌中,63 例(35%)有 KRAS 突变(KRAS+),35 例(19%)有 EGFR 突变(EGFR+),82 例(46%)无突变(KRAS-/EGFR-)。在 KRAS+癌中,实性生长模式明显更为常见:KRAS+癌中实性模式的平均值±标准差为 27±34%,而 EGFR+癌中为 3±10%(P<0.001),KRAS-/EGFR-癌中为 15±27%(P=0.033)。此外,在 KRAS+(28/63;44%)中至少局灶性(≥20%)的实性成分比 EGFR+(2/35;6%;P<0.001)和 KRAS-/EGFR-(21/82;26%;P=0.022)癌中更常见。KRAS 突变也在黏液型癌中过度表达,并且与肿瘤浸润白细胞和更重的吸烟史显著相关。EGFR 突变与非黏液性非实性模式相关,特别是贴壁型和乳头状,无坏死,无细胞学异型性,鞋钉状细胞,TTF-1 表达,从不/轻度吸烟史。总之,对肺腺癌的扩展分子和临床病理分析揭示了 KRAS 突变与实体组织学和肿瘤浸润性炎症细胞之间的新关联,并扩展了先前认识到的 KRAS 和 EGFR 突变的几种形态和临床关联。最近已经证明,实体生长模式是肺腺癌侵袭性行为的强有力预测因子,这可能是这些肿瘤中与 KRAS 突变相关的不良预后的基础。