Section of Oncology, Department of Clinical Science, University of Bergen, Bergen, Norway.
Endocr Relat Cancer. 2013 Jun 24;20(4):R183-201. doi: 10.1530/ERC-13-0099. Print 2013 Aug.
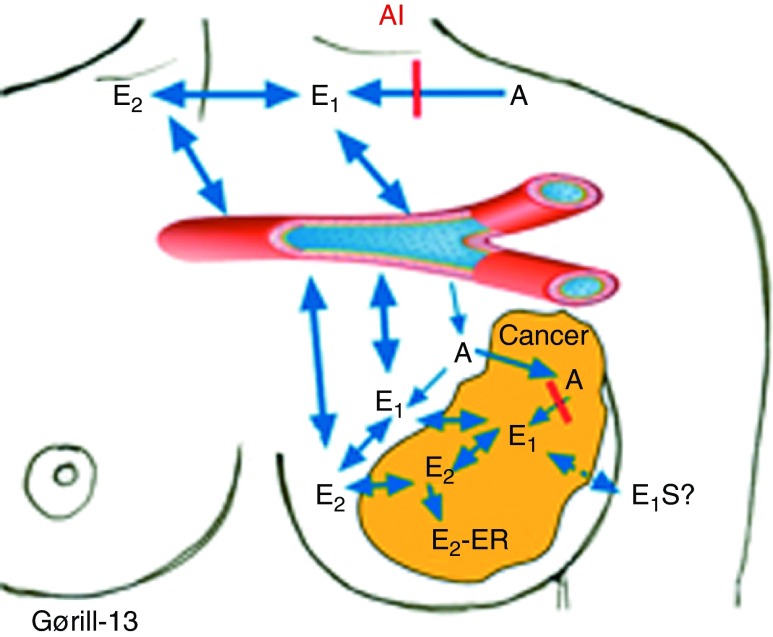
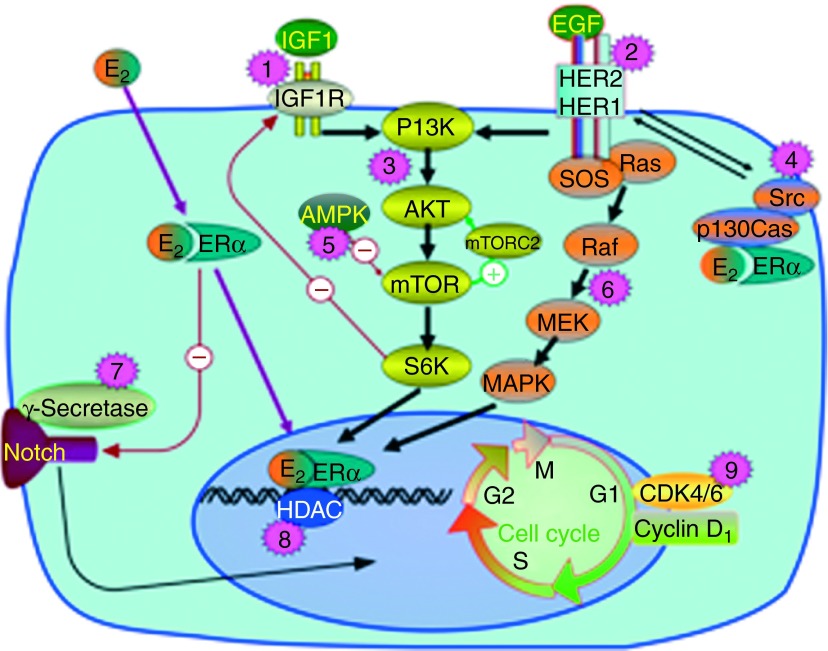
Following their successful implementation for the treatment of metastatic breast cancer, the 'third-generation' aromatase inhibitors (anastrozole, letrozole, and exemestane) have now become standard adjuvant endocrine treatment for postmenopausal estrogen receptor-positive breast cancers. These drugs are characterized by potent aromatase inhibition, causing >98% inhibition of estrogen synthesis in vivo. A recent meta-analysis found no difference in anti-tumor efficacy between these three compounds. As of today, aromatase inhibitor monotherapy and sequential treatment using tamoxifen followed by an aromatase inhibitor for a total of 5 years are considered equipotent treatment options. However, current trials are addressing the potential benefit of extending treatment duration beyond 5 years. Regarding side effects, aromatase inhibitors are not found associated with enhanced risk of cardiovascular disease, and enhanced bone loss is prevented by adding bisphosphonates in concert for those at danger of developing osteoporosis. However, arthralgia and carpal tunnel syndrome preclude drug administration among a few patients. While recent findings have questioned the use of aromatase inhibitors among overweight and, in particular, obese patients, this problem seems to focus on premenopausal patients treated with an aromatase inhibitor and an LH-RH analog in concert, questioning the efficacy of LH-RH analogs rather than aromatase inhibitors among overweight patients. Finally, recent findings revealing a benefit from adding the mTOR inhibitor everolimus to endocrine treatment indicate targeted therapy against defined growth factor pathways to be a way forward, by reversing acquired resistance to endocrine therapy.
继成功用于转移性乳腺癌的治疗后,第三代芳香酶抑制剂(阿那曲唑、来曲唑和依西美坦)现已成为绝经后雌激素受体阳性乳腺癌的标准辅助内分泌治疗药物。这些药物的特点是具有强大的芳香酶抑制作用,在体内可使雌激素合成抑制>98%。最近的一项荟萃分析发现这三种化合物的抗肿瘤疗效没有差异。截至今日,芳香酶抑制剂单药治疗和序贯治疗,即先用他莫昔芬治疗,然后再用芳香酶抑制剂治疗,总疗程为 5 年,被认为是等效的治疗选择。然而,目前的试验正在探讨将治疗时间延长至 5 年以上的潜在获益。关于副作用,芳香酶抑制剂与心血管疾病风险增加无关,而且通过联合使用双磷酸盐,可以预防骨质流失,从而为那些有发生骨质疏松风险的患者提供保护。然而,关节痛和腕管综合征会使少数患者无法进行药物治疗。虽然最近的研究结果对超重患者,尤其是肥胖患者使用芳香酶抑制剂提出了质疑,但这个问题似乎主要集中在接受芳香酶抑制剂和 LH-RH 类似物联合治疗的绝经前患者身上,质疑的是 LH-RH 类似物而非超重患者的芳香酶抑制剂的疗效。最后,最近的研究结果表明,在内分泌治疗中加入 mTOR 抑制剂依维莫司可获益,这表明针对特定生长因子通路的靶向治疗可能是一种可行的方法,可逆转对内分泌治疗的获得性耐药。