Department of Surgical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA.
J Am Coll Surg. 2013 Jul;217(1):126-33; discussion 133-4. doi: 10.1016/j.jamcollsurg.2013.03.004. Epub 2013 Apr 28.
The primary reported indication for the associating liver partition with portal vein ligation for staged hepatectomy (ALPPS) technique is in patients with very low future liver remnant volumes. Given the elevated incidence of major morbidity (40%) and liver-related mortality (12%) with ALPPS, we sought to determine the safety and efficacy of percutaneous portal vein embolization (PVE) in a similar patient population.
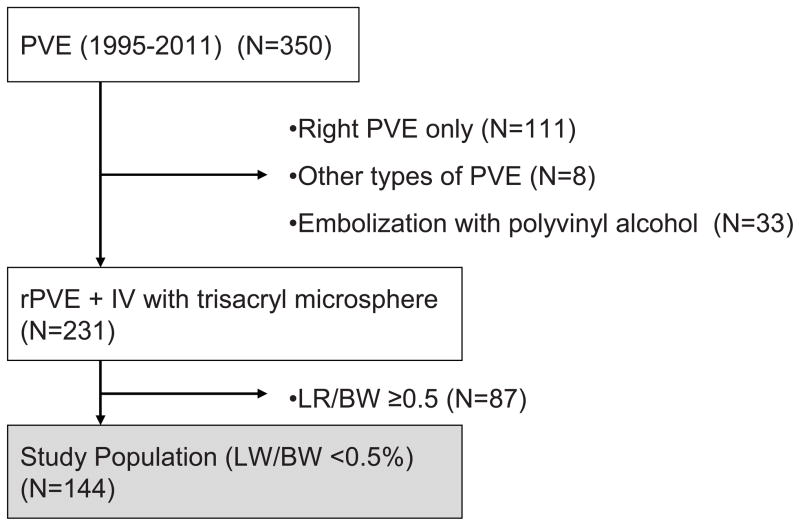
Tumor resectability and morbidity and mortality rates were reviewed for 144 consecutive liver tumor patients with future liver remnant to body weight ratios (LR/BW) less than 0.5%. All patients were referred for preoperative percutaneous right plus segment IV PVE using embolic microspheres, with planned reassessment of the LR/BW 30 days after PVE. Post-PVE outcomes were compared with reported outcomes for ALPPS.
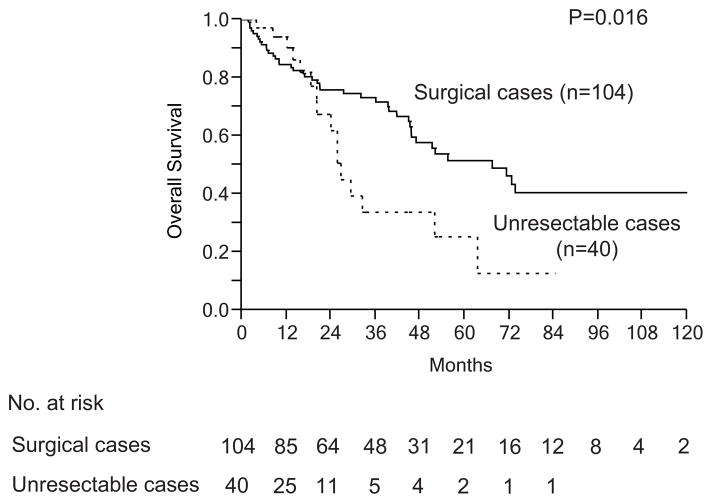
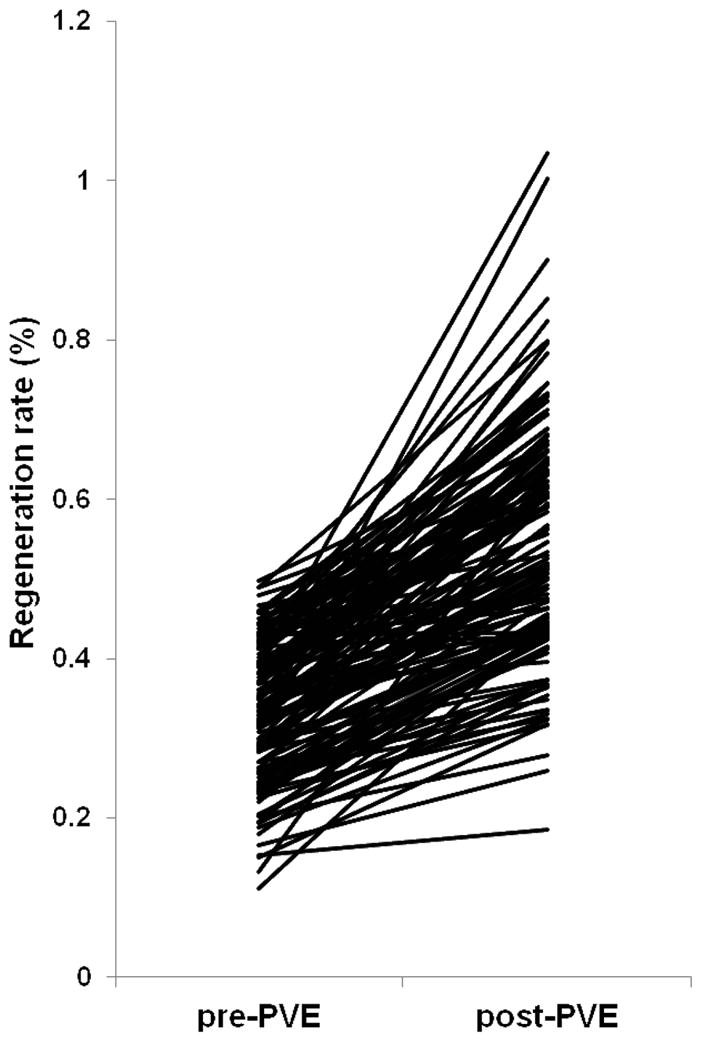
Percutaneous PVE was successfully performed in 141 of the 144 study patients (97.9%). Adequate regeneration was observed in 139 patients (98.5%) with median post-PVE LR/BW rising from 0.33% to 0.52% (p < 0.0001), representing a per-patient median regeneration rate of 62% (range 0.3% to 379%). In total, 104 patients underwent extended right hepatectomy (n = 102) or right hepatectomy (n = 2). The remaining 40 patients (27.8%) were not resectable due to short-interval disease progression (27 patients, 18.5%), insufficient liver regeneration (5 patients, 3.5%), and medical comorbidities (8 patients, 5.6%). After resection, the following outcomes were observed: major morbidity: 33.0% (34 of 104), liver insufficiency: 12.5% (13 of 104), and 90-day liver-related mortality: 5.8% (6 of 104). These oncologic and technical results compare favorably with those of ALPPS.
Based on its ability to select oncologically resectable patients and superior safety and efficacy profiles, percutaneous right + segment IV PVE and interval surgery remains the standard of care for patients with very low future liver remnant volumes.
联合肝脏离断和门静脉结扎的二步肝切除术(ALPPS)技术的主要适应证是未来肝残留体积非常低的患者。鉴于 ALPPS 的主要发病率(40%)和与肝脏相关的死亡率(12%)较高,我们试图确定经皮门静脉栓塞术(PVE)在类似患者人群中的安全性和有效性。
回顾了 144 例连续肝肿瘤患者的肿瘤可切除性和发病率及死亡率,这些患者的未来肝残留与体重比(LR/BW)小于 0.5%。所有患者均接受经皮右叶加 IV 段 PVE 治疗,使用栓塞微球,计划在 PVE 后 30 天重新评估 LR/BW。比较经皮 PVE 后的结果与 ALPPS 的报告结果。
144 例研究患者中有 141 例(97.9%)成功进行了经皮 PVE。139 例(98.5%)患者观察到充分再生,中位 PVE 后 LR/BW 从 0.33%上升至 0.52%(p<0.0001),代表每位患者的中位再生率为 62%(范围 0.3%至 379%)。总共 104 例患者接受了扩大右肝切除术(n=102)或右半肝切除术(n=2)。其余 40 例(27.8%)因短间隔疾病进展(27 例,18.5%)、肝再生不足(5 例,3.5%)和医疗合并症(8 例,5.6%)而无法切除。切除后观察到以下结果:主要发病率:33.0%(34/104),肝功能不全:12.5%(13/104),90 天与肝脏相关的死亡率:5.8%(6/104)。这些肿瘤学和技术结果与 ALPPS 相比具有优势。
基于其选择肿瘤可切除患者的能力以及更高的安全性和有效性,经皮右叶+IV 段 PVE 和间隔手术仍然是未来肝残留体积非常低的患者的标准治疗方法。