John Wayne Cancer Institute, Santa Monica, the Partnership for Health Analytic Research, LLC, Beverly Hills, the Keck School of Medicine at the University of Southern California, Los Angeles, and the Department of Obstetrics & Gynecology, Stanford University School of Medicine, Stanford Women's Cancer Center, Stanford Cancer Institute, Stanford, California; the Channing Division of Network Medicine, Department of Medicine, and the Division of Preventive Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts; and the University of Auckland, Auckland, New Zealand.
Obstet Gynecol. 2013 Apr;121(4):709-716. doi: 10.1097/AOG.0b013e3182864350.
To report long-term mortality after oophorectomy or ovarian conservation at the time of hysterectomy in subgroups of women based on age at the time of surgery, use of estrogen therapy, presence of risk factors for coronary heart disease, and length of follow-up.
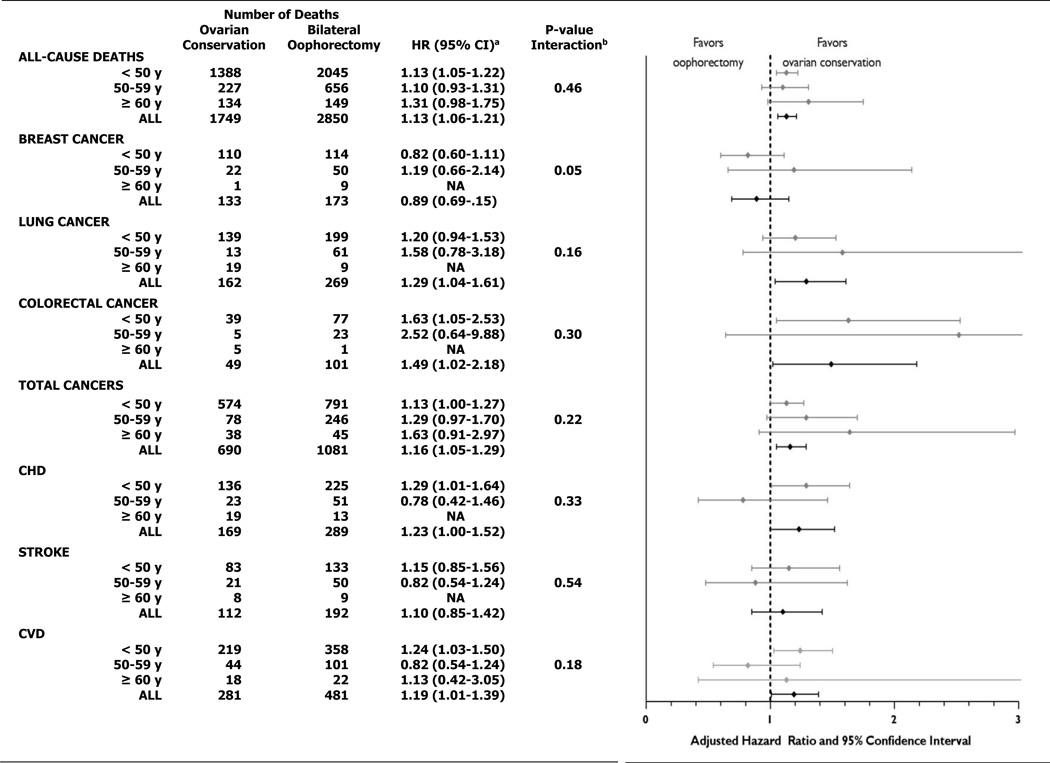
This was a prospective cohort study of 30,117 Nurses' Health Study participants undergoing hysterectomy for benign disease. Multivariable adjusted hazard ratios for death from coronary heart disease, stroke, breast cancer, epithelial ovarian cancer, lung cancer, colorectal cancer, total cancer, and all causes were determined comparing bilateral oophorectomy (n=16,914) with ovarian conservation (n=13,203).
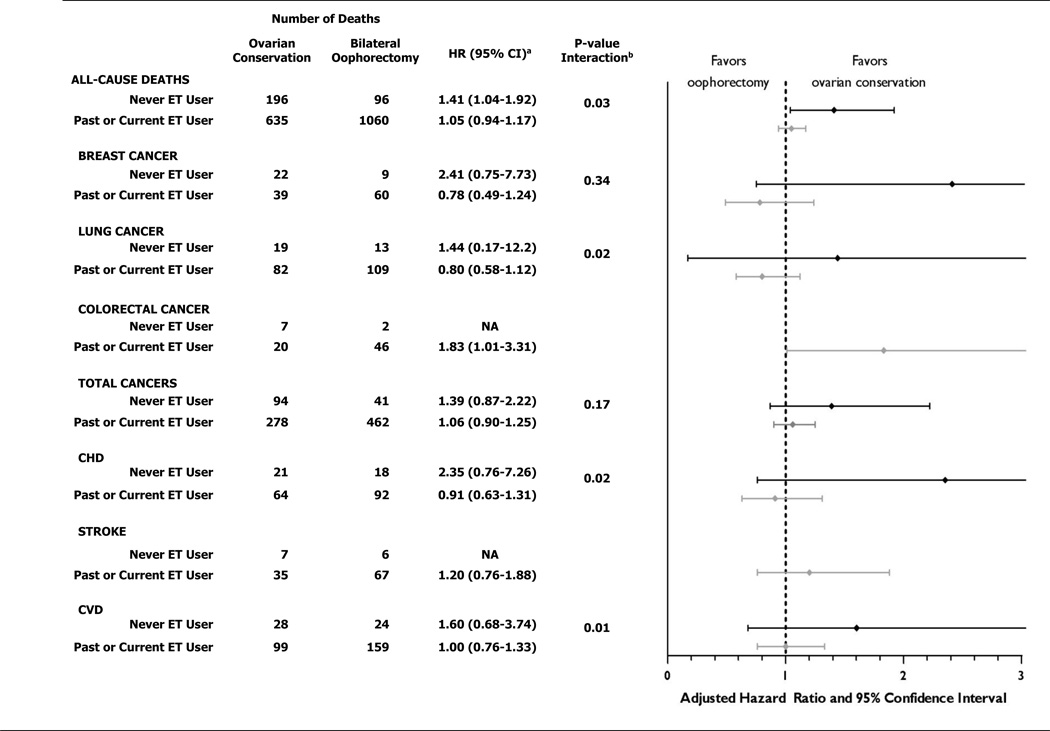
Over 28 years of follow-up, 16.8% of women with hysterectomy and bilateral oophorectomy died from all causes compared with 13.3% of women who had ovarian conservation (hazard ratio 1.13, 95% confidence interval 1.06-1.21). Oophorectomy was associated with a lower risk of death from ovarian cancer (four women with oophorectomy compared with 44 women with ovarian conservation) and, before age 47.5 years, a lower risk of death from breast cancer. However, at no age was oophorectomy associated with a lower risk of other cause-specific or all-cause mortality. For women younger than 50 years at the time of hysterectomy, bilateral oophorectomy was associated with significantly increased mortality in women who had never used estrogen therapy but not in past and current users: assuming a 35-year lifespan after oophorectomy: number needed to harm for all-cause death=8, coronary heart disease death=33, and lung cancer death=50.
Bilateral oophorectomy is associated with increased mortality in women aged younger than 50 years who never used estrogen therapy and at no age is oophorectomy associated with increased survival.
I.
根据手术时的年龄、雌激素治疗的使用情况、冠心病危险因素的存在以及随访时间的长短,在基于手术时年龄、雌激素治疗的使用情况、冠心病危险因素的存在以及随访时间长短的亚组妇女中,报告卵巢切除术或子宫切除术时卵巢保留的长期死亡率。
这是一项对 30117 名参加护士健康研究的妇女进行的前瞻性队列研究,这些妇女因良性疾病接受了子宫切除术。通过比较双侧卵巢切除术(n=16914)与卵巢保留术(n=13203),确定了因冠心病、中风、乳腺癌、上皮性卵巢癌、肺癌、结直肠癌、总癌症和所有原因死亡的多变量调整风险比。
在 28 年的随访中,与卵巢保留的妇女(133%)相比,接受子宫切除术和双侧卵巢切除术的妇女中有 16.8%死于所有原因(风险比 1.13,95%置信区间 1.06-1.21)。卵巢切除术与卵巢癌死亡风险降低相关(4 例卵巢切除术患者与 44 例卵巢保留术患者相比),并且在 47.5 岁之前,乳腺癌死亡风险降低。然而,在任何年龄,卵巢切除术与其他特定原因或所有原因死亡率降低均无关。对于在子宫切除术时年龄小于 50 岁的妇女,双侧卵巢切除术与从未使用雌激素治疗的妇女的死亡率显著增加相关,但与过去和现在使用雌激素治疗的妇女无关:假设卵巢切除术后有 35 年的寿命:全因死亡的需要伤害人数=8,冠心病死亡人数=33,肺癌死亡人数=50。
双侧卵巢切除术与从未使用雌激素治疗的年龄小于 50 岁的妇女的死亡率增加相关,并且在任何年龄,卵巢切除术均与生存率增加无关。
I。