Department of Emergency Medicine, University of Mississippi School of Medicine, Jackson, Mississippi 39216, USA.
Shock. 2013 Jul;40(1):11-4. doi: 10.1097/SHK.0b013e318298836d.
The current consensus definition of septic shock requires hypotension after adequate fluid challenge or vasopressor requirement. Some patients with septic shock present with hypotension and hyperlactatemia greater than 2 mmol/L (tissue dysoxic shock), whereas others have hypotension alone with normal lactate (vasoplegic shock).
The objective of this study was to determine differences in outcomes of patients with tissue dysoxic versus vasoplegic septic shock.
This was a secondary analysis of a large, multicenter randomized controlled trial. Inclusion criteria were suspected infection, two or more systemic inflammatory response criteria, and systolic blood pressure less than 90 mmHg after a fluid bolus. Patients were categorized by presence of vasoplegic or tissue dysoxic shock. Demographics and Sequential Organ Failure Assessment scores were evaluated between the groups. The primary outcome was in-hospital mortality.
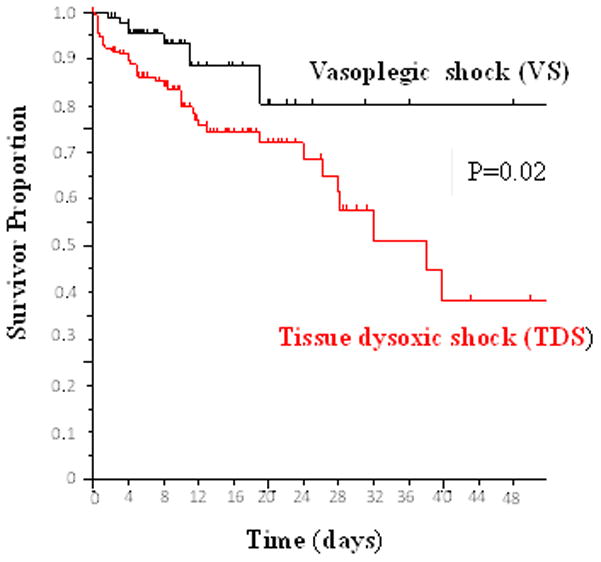
A total of 247 patients were included, 90 patients with vasoplegic shock and 157 with tissue dysoxic shock. There were no significant differences in age, race, or sex between the vasoplegic and tissue dysoxic shock groups. The group with vasoplegic shock had a lower initial Sequential Organ Failure Assessment score than did the group with tissue dysoxic shock (5.5 vs. 7.0 points; P = 0.0002). The primary outcome of in-hospital mortality occurred in 8 (9%) of 90 patients with vasoplegic shock compared with 41 (26%) of 157 in the group with tissue dysoxic shock (proportion difference, 17%; 95% confidence interval, 7%-26%; P < 0.0001; log-rank test P = 0.02). After adjusting for confounders, tissue dysoxic shock remained an independent predictor of in-hospital mortality.
In this analysis of patients with septic shock, we found a significant difference in in-hospital mortality between patients with vasoplegic versus tissue dysoxic septic shock. These findings suggest a need to consider these differences when designing future studies of septic shock therapies.
目前,感染性休克的共识定义需要在充分液体复苏或血管加压药治疗后出现低血压。一些感染性休克患者表现为低血压和大于 2mmol/L 的高乳酸血症(组织缺氧性休克),而另一些患者仅表现为低血压和正常乳酸血症(血管扩张性休克)。
本研究旨在确定组织缺氧性与血管扩张性感染性休克患者结局的差异。
这是一项大型多中心随机对照试验的二次分析。纳入标准为疑似感染、存在两个或更多全身炎症反应标准以及液体复苏后收缩压低于 90mmHg。根据是否存在血管扩张性或组织缺氧性休克对患者进行分类。评估两组间的人口统计学和序贯器官衰竭评估评分。主要结局为住院死亡率。
共纳入 247 例患者,90 例为血管扩张性休克,157 例为组织缺氧性休克。血管扩张性和组织缺氧性休克组间的年龄、种族和性别无显著差异。血管扩张性休克组的初始序贯器官衰竭评估评分低于组织缺氧性休克组(5.5 分 vs. 7.0 分;P=0.0002)。血管扩张性休克组的住院死亡率为 8(9%)例,组织缺氧性休克组为 41(26%)例(比例差异为 17%;95%置信区间为 7%-26%;P<0.0001;对数秩检验 P=0.02)。调整混杂因素后,组织缺氧性休克仍然是住院死亡率的独立预测因素。
在这项感染性休克患者的分析中,我们发现血管扩张性与组织缺氧性感染性休克患者的住院死亡率存在显著差异。这些发现表明,在设计未来的感染性休克治疗研究时,需要考虑这些差异。