Centre for Integrated Critical Care, Department of Medicine & Radiology, The University of Melbourne, Melbourne, Victoria, Australia.
Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia.
Am J Respir Crit Care Med. 2020 Nov 1;202(9):1253-1261. doi: 10.1164/rccm.201911-2172OC.
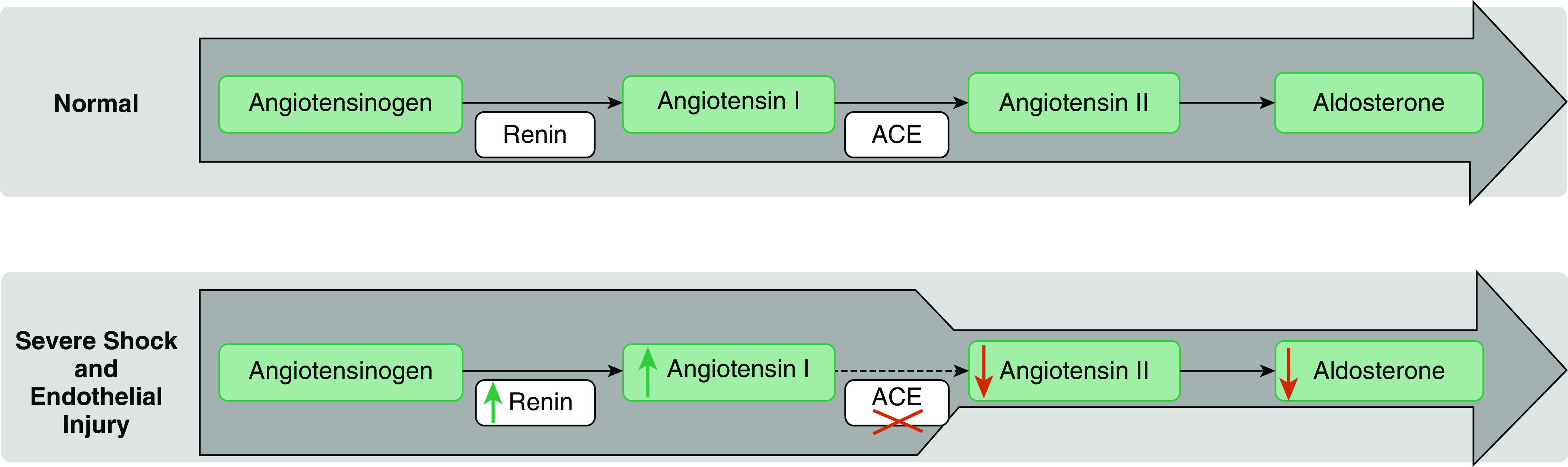
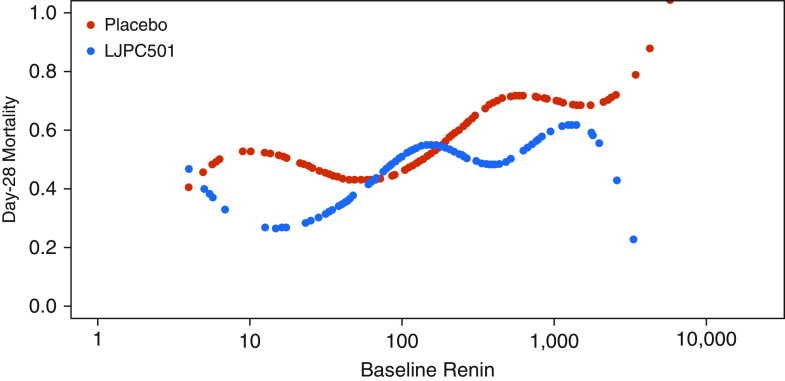
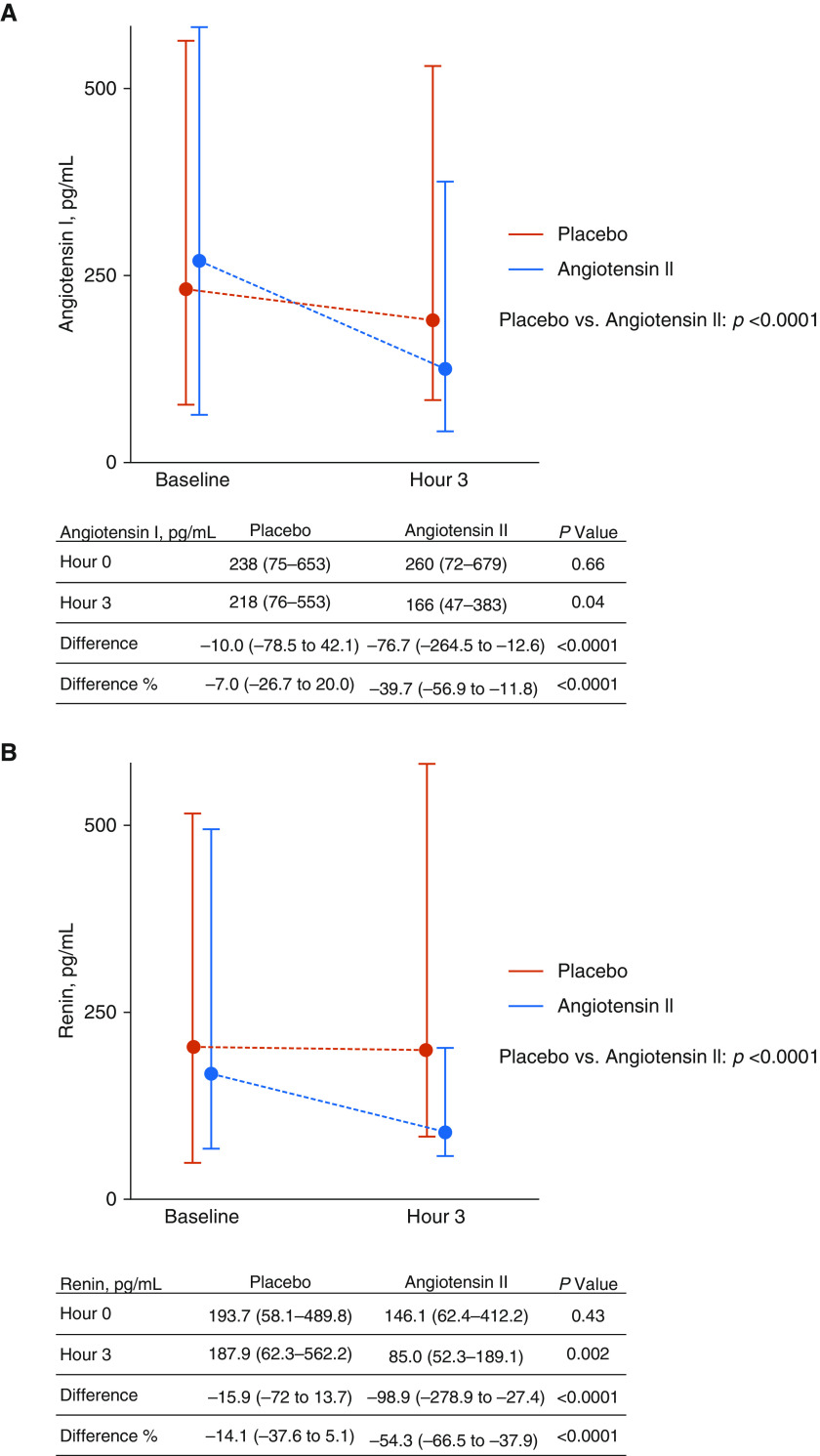
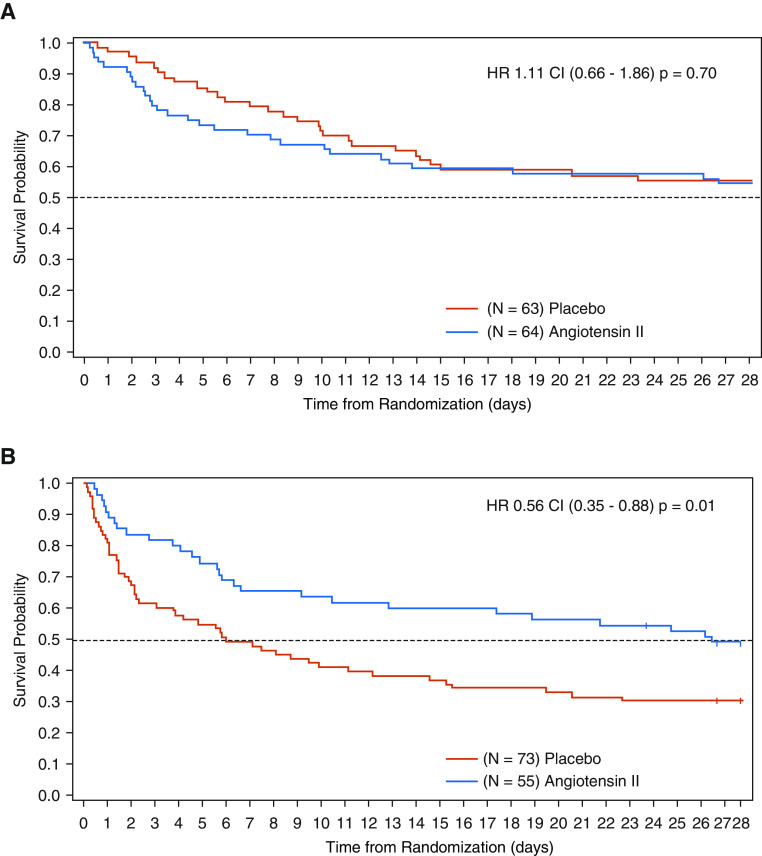
Exogenous angiotensin II increases mean arterial pressure in patients with catecholamine-resistant vasodilatory shock (CRVS). We hypothesized that renin concentrations may identify patients most likely to benefit from such therapy. To test the kinetic changes in renin concentrations and their prognostic value in patients with CRVS. We analyzed serum samples from patients enrolled in the ATHOS-3 (Angiotensin II for the Treatment of High-Output Shock) trial for renin, angiotensin I, and angiotensin II concentrations before the start of administration of angiotensin II or placebo and after 3 hours. Baseline serum renin concentration (normal range, 2.13-58.78 pg/ml) was above the upper limits of normal in 194 of 255 (76%) study patients with a median renin concentration of 172.7 pg/ml (interquartile range [IQR], 60.7 to 440.6 pg/ml), approximately threefold higher than the upper limit of normal. Renin concentrations correlated positively with angiotensin I/II ratios ( = 0.39; < 0.001). At 3 hours after initiation of angiotensin II therapy, there was a 54.3% reduction (IQR, 37.9% to 66.5% reduction) in renin concentration compared with a 14.1% reduction (IQR, 37.6% reduction to 5.1% increase) with placebo ( < 0.0001). In patients with renin concentrations above the study population median, angiotensin II significantly reduced 28-day mortality to 28 of 55 (50.9%) patients compared with 51 of 73 patients (69.9%) treated with placebo (unstratified hazard ratio, 0.56; 95% confidence interval, 0.35 to 0.88; = 0.012) ( = 0.048 for the interaction). The serum renin concentration is markedly elevated in CRVS and may identify patients for whom treatment with angiotensin II has a beneficial effect on clinical outcomes.Clinical trial registered with www.clinicaltrials.gov (NCT02338843).
外源性血管紧张素 II 可增加儿茶酚胺抵抗性血管扩张性休克(CRVS)患者的平均动脉压。我们假设肾素浓度可能可以识别最有可能从这种治疗中受益的患者。为了测试 CRVS 患者肾素浓度的动力学变化及其预后价值,我们分析了 ATHOS-3(血管紧张素 II 治疗高输出休克)试验中纳入的患者的血清样本,以确定肾素、血管紧张素 I 和血管紧张素 II 浓度在开始使用血管紧张素 II 或安慰剂之前和之后 3 小时的浓度。在 255 名研究患者中,有 194 名(76%)患者的基础血清肾素浓度高于正常范围(正常范围为 2.13-58.78pg/ml),中位数为 172.7pg/ml(四分位距[IQR],60.7-440.6pg/ml),大约是正常上限的三倍。肾素浓度与血管紧张素 I/II 比值呈正相关( = 0.39; < 0.001)。在开始血管紧张素 II 治疗后 3 小时,与安慰剂相比,肾素浓度降低了 54.3%(IQR,37.9%至 66.5%降低),而降低了 14.1%(IQR,37.6%降低至 5.1%增加)( < 0.0001)。在肾素浓度高于研究人群中位数的患者中,与安慰剂组相比,血管紧张素 II 显著降低了 28 天死亡率,从 55 名患者中的 28 名(50.9%)降至 73 名患者中的 51 名(69.9%)(未分层危险比,0.56;95%置信区间,0.35 至 0.88; = 0.012)( = 0.048 用于交互作用)。CRVS 患者的血清肾素浓度明显升高,可能可以识别出那些接受血管紧张素 II 治疗对临床结局有有益影响的患者。临床试验在 www.clinicaltrials.gov 注册(NCT02338843)。