Children's Hospital, Pakistan Institute of Medical Sciences, Islamabad, Pakistan.
PLoS Med. 2013;10(5):e1001422. doi: 10.1371/journal.pmed.1001422. Epub 2013 May 7.
Antibiotic treatment for pneumonia as measured by Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS) is a key indicator for tracking progress in achieving Millennium Development Goal 4. Concerns about the validity of this indicator led us to perform an evaluation in urban and rural settings in Pakistan and Bangladesh.
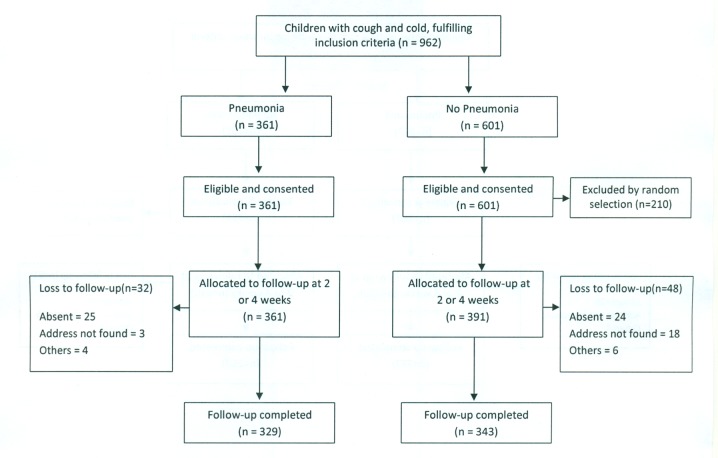
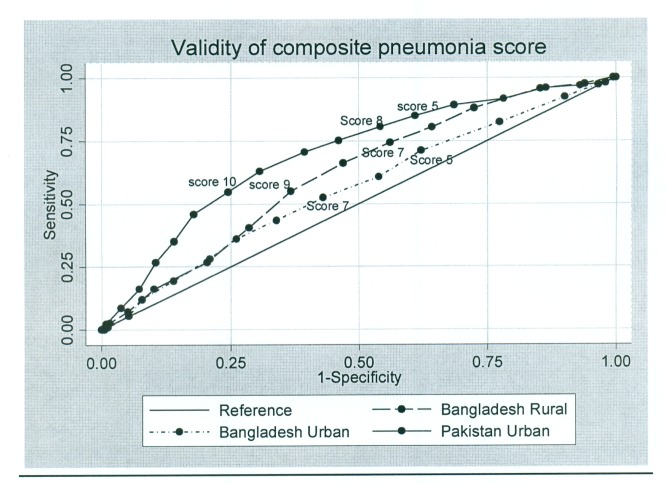
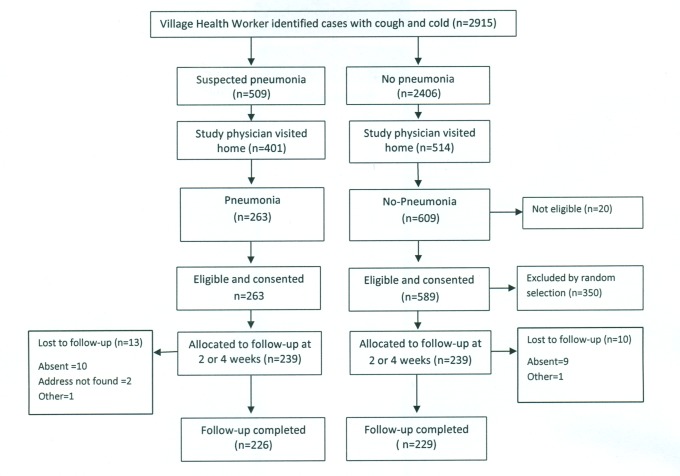
Caregivers of 950 children under 5 y with pneumonia and 980 with "no pneumonia" were identified in urban and rural settings and allocated for DHS/MICS questions 2 or 4 wk later. Study physicians assigned a diagnosis of pneumonia as reference standard; the predictive ability of DHS/MICS questions and additional measurement tools to identify pneumonia versus non-pneumonia cases was evaluated. Results at both sites showed suboptimal discriminative power, with no difference between 2- or 4-wk recall. Individual patterns of sensitivity and specificity varied substantially across study sites (sensitivity 66.9% and 45.5%, and specificity 68.8% and 69.5%, for DHS in Pakistan and Bangladesh, respectively). Prescribed antibiotics for pneumonia were correctly recalled by about two-thirds of caregivers using DHS questions, increasing to 72% and 82% in Pakistan and Bangladesh, respectively, using a drug chart and detailed enquiry.
Monitoring antibiotic treatment of pneumonia is essential for national and global programs. Current (DHS/MICS questions) and proposed new (video and pneumonia score) methods of identifying pneumonia based on maternal recall discriminate poorly between pneumonia and children with cough. Furthermore, these methods have a low yield to identify children who have true pneumonia. Reported antibiotic treatment rates among these children are therefore not a valid proxy indicator of pneumonia treatment rates. These results have important implications for program monitoring and suggest that data in its current format from DHS/MICS surveys should not be used for the purpose of monitoring antibiotic treatment rates in children with pneumonia at the present time.
通过人口与健康调查(DHS)和多指标类集调查(MICS)来衡量肺炎的抗生素治疗,是跟踪实现千年发展目标 4 进展的关键指标。由于对该指标的有效性存在担忧,我们在巴基斯坦和孟加拉国的城乡地区进行了评估。
在城乡地区确定了 950 名 5 岁以下患有肺炎的儿童和 980 名“无肺炎”的儿童的看护者,并在 2 或 4 周后为其分配 DHS/MICS 问题。研究医生将肺炎诊断作为参考标准;评估了 DHS/MICS 问题和其他测量工具来识别肺炎与非肺炎病例的预测能力。两个地点的结果均显示出较差的区分能力,2 周和 4 周回忆之间没有差异。各研究地点的敏感性和特异性个体模式差异很大(在巴基斯坦和孟加拉国,DHS 的敏感性分别为 66.9%和 45.5%,特异性分别为 68.8%和 69.5%)。约有三分之二的看护者使用 DHS 问题正确回忆了肺炎的抗生素治疗,而在巴基斯坦和孟加拉国,分别使用药物图表和详细询问,这一比例增加到 72%和 82%。
监测肺炎的抗生素治疗对于国家和全球计划至关重要。目前(DHS/MICS 问题)和提议的新方法(视频和肺炎评分)基于母亲回忆来识别肺炎,在区分肺炎和咳嗽儿童方面效果不佳。此外,这些方法对确定真正患有肺炎的儿童的效果不佳。因此,这些儿童报告的抗生素治疗率并不是肺炎治疗率的有效替代指标。这些结果对计划监测具有重要意义,并表明目前 DHS/MICS 调查的数据格式不应用于监测当前儿童肺炎的抗生素治疗率。