Ferring International PharmaScience Center, Kay Fiskers Plads 11, 2300 Copenhagen, Denmark.
Eur J Pediatr. 2013 Sep;172(9):1235-42. doi: 10.1007/s00431-013-1992-9. Epub 2013 May 16.
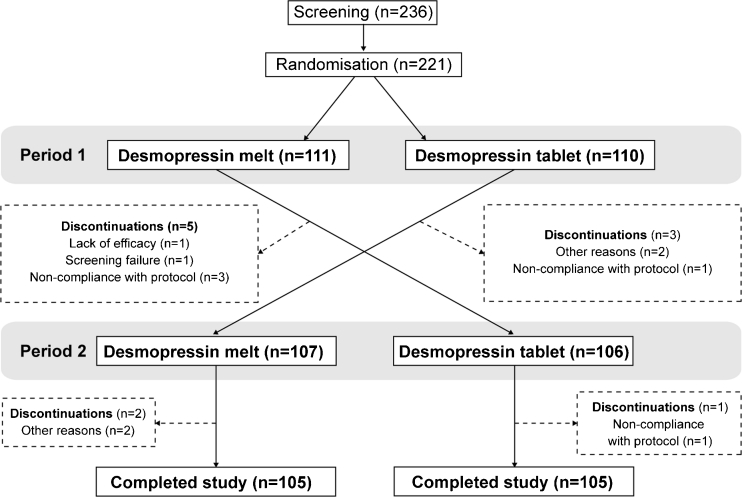
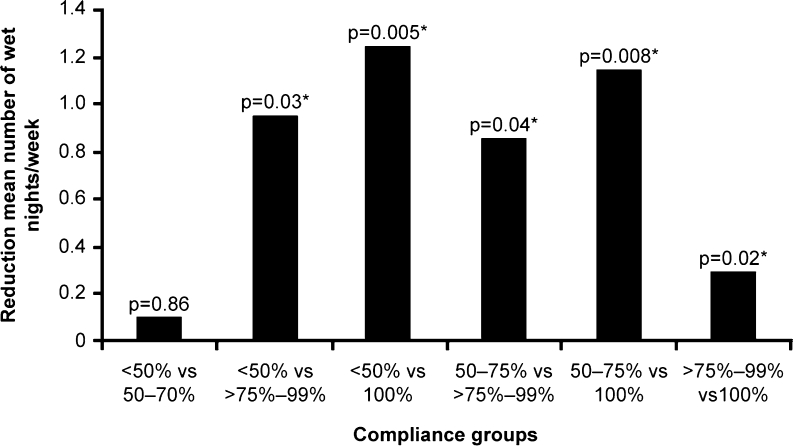
Primary nocturnal enuresis is a prevalent childhood condition that can persist into adulthood. Desmopressin is an antidiuretic available as orally disintegrating lyophilisate (melt) or solid tablet. Recent findings suggesting different food interactions and clinical characteristics, including compliance, between desmopressin melt and tablet motivated a post hoc analysis of a previously reported randomised, crossover study. The efficacy of desmopressin melt compared with tablet was evaluated using the International Children's Continence Society (ICCS) responder definitions. Compliance was further analysed using detailed criteria, and the association between efficacy and compliance was examined. In total, 221 patients aged 5-15 years, already receiving desmopressin tablets were randomised to the treatment sequence melt (120/240 μg)/tablet (0.2/0.4 mg) or tablet/melt in two consecutive 3-week periods. The probability of being a responder (partial or full) during either period was significantly more likely with desmopressin melt compared with tablet (odds ratio, 2.0; confidence intervals, 1.07-3.73; p = 0.03). There was no period effect on compliance in the tablet/melt sequence and no difference in the number of completely compliant patients in each formulation group; however, more patients were >75 % compliant in period 1 compared with period 2 in the melt/tablet sequence. Increased compliance was associated with greater reductions in the number of wet nights for both formulations.
Desmopressin melt, compared with tablet, improves the probability of being a responder. Switching from tablet to melt formulation increased patient compliance. Increased compliance was associated with increased efficacy. Switching to desmopressin melt may benefit patients with suboptimal responses to desmopressin tablet.
原发性夜间遗尿症是一种普遍的儿童疾病,可能持续到成年期。去氨加压素是一种抗利尿药,有口服崩解冻干(溶解)和固体片剂两种形式。最近的研究结果表明,去氨加压素溶解片和片剂在食物相互作用和临床特征(包括顺应性)方面存在差异,这促使我们对之前报告的一项随机交叉研究进行了事后分析。去氨加压素溶解片与片剂的疗效比较采用国际儿童尿控协会(ICCS)应答定义进行评估。进一步使用详细标准分析顺应性,并检查疗效与顺应性之间的关系。共有 221 名年龄在 5-15 岁、已接受去氨加压素片剂治疗的患者被随机分配至接受治疗顺序为溶解片(120/240μg)/片剂(0.2/0.4mg)或片剂/溶解片,两种方案连续治疗 3 周。在任一治疗期,与片剂相比,使用去氨加压素溶解片更有可能成为部分或完全应答者(优势比,2.0;置信区间,1.07-3.73;p=0.03)。在片剂/溶解片顺序中,顺应性没有周期效应,两种制剂组完全顺应的患者数量也没有差异;然而,在溶解片/片剂顺序中,更多的患者在第 1 期比第 2 期的顺应性>75%。两种制剂的顺应性增加都与夜间湿尿次数的减少量更大有关。
与片剂相比,去氨加压素溶解片提高了成为应答者的可能性。从片剂转换为溶解片制剂提高了患者的顺应性。增加的顺应性与更高的疗效相关。转换为去氨加压素溶解片可能有益于对去氨加压素片剂反应不佳的患者。